

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Confluent and reticulated papillomatosis (CRP) is an uncommon progressive and distinctive dermatosis characterized by persistent brown, scaly macules, papules, patches, and plaques. It was first described in 1927 by Gougerot and Carteaud as “papillomatoses pigmentée innominée”; later, they renamed it “papillomatoses pigmentée confluente et réticulée”1. It was subsequently categorized as a new form of cutaneous papillomatosis, and its diagnostic criteria were established. Wise and Sachs2 described the first case in the United States in 1937 and called it confluent and reticular papillomatosis. CRP is a rare dermatosis of an uncertain etiology that typically affects young adults, especially in the middle of the chest and back. It may simulate pigmented tinea versicolor, acanthosis nigricans (AN), or epidermal nevus3. The histopathology of CRP involves orthohyperkeratosis, papillomatosis, minimal to mild acanthosis, and usually no significant inflammatory infiltrate. Although it has a chronic course, spontaneous resolution with subsequent recurrence can also occur4. The aims of this study were as follows. First, because CRP is known to occur predominantly in teenage patients5, it is necessary to clarify the histopathologic differences between teenage and adult patients. Second, studies on CRP in Asia, especially in Korea, are lacking. Based on the results of this study, differences between age groups can be identified, and information on Korean patients with CRP can be provided.
MATERIALS AND METHODS
Subjects
We retrospectively reviewed the medical records, clinical photographs, and 40 histopathologic slides of 29 patients diagnosed with CRP between July 2009 and June 2016 after receiving approval from the Institutional Review Board of the affiliated Eulji University Hospital (IRB no. 2016-12-040). Based on a cut-off age of 18 years, we divided the patients into the adolescent and adult groups to compare the clinical and histopathologic findings by the anatomic site. We received the patient's consent form about publishing all photographic materials.
Histopathology
Forty biopsy samples (adolescent group, 21; adult group, 19) obtained from 29 patients were stained with hematoxylin and eosin and reviewed by one pathologist and two dermatologists. Hyperkeratosis, parakeratosis, acanthosis, and papillomatosis in the epidermis were evaluated. We used a four-point scale (0, not visible; 1, mild; 2, moderate; and 3, severe) to assess each item. The density of the infiltrated inflammatory cells in the dermis was evaluated.
RESULTS
Patients' demographic characteristics
1) Age distribution
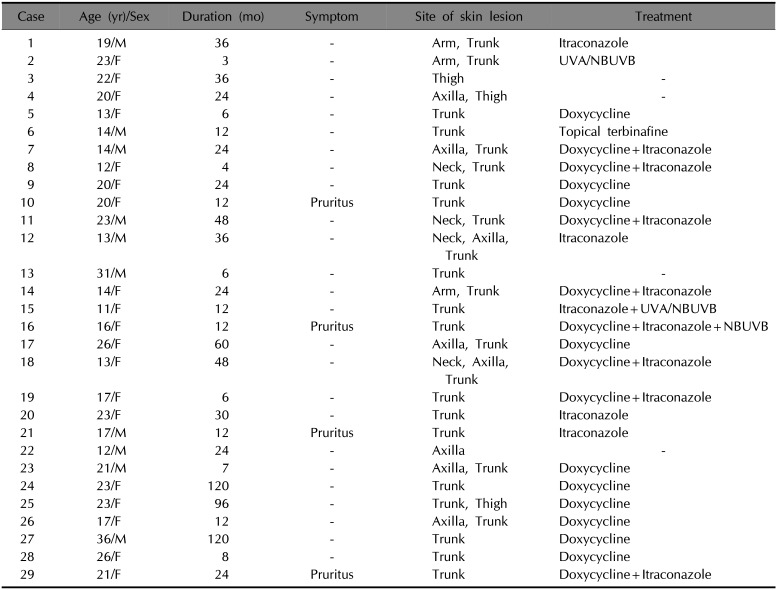
Among the total of 29 patients with CRP, 13 were aged 1~18 years (adolescent group: age range, 12~17 years), and 16 were aged >18 years (adult group: age range, 19~36 years). The mean age of the entire cohort was 19.3 years, while those of the adolescent and adult groups were 14.1 years and 23.6 years, respectively (Table 1).
2) Sex ratio (male:female) and age at onset
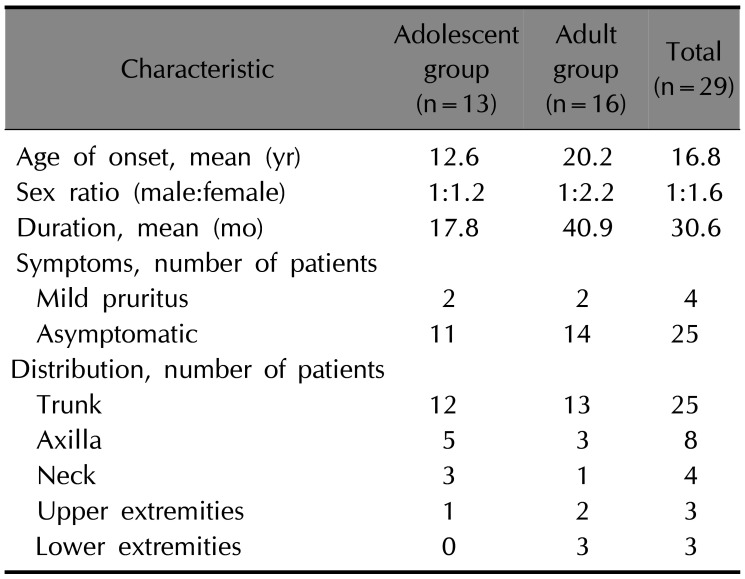
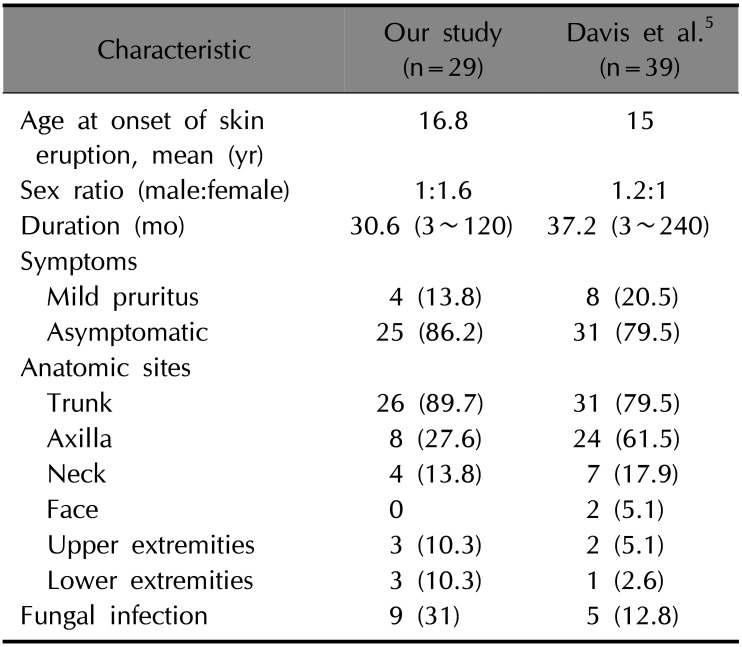
Eleven men and 18 women participated. The male-to-female sex ratio was 1:1.6 in all patients, 1:1.2 in the adolescent group, and 1:2.2 in the adult group. The mean age at onset was 16.8 years in all patients, 12.6 years in the adolescent group, and 20.2 years in the adult group (Table 2).
4) Clinical characteristics
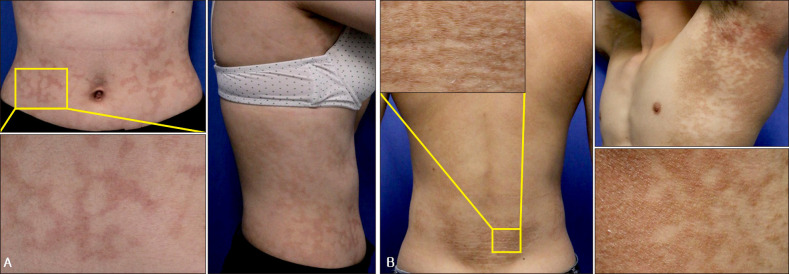
Four patients (two in the adolescent group and two in the adult group) reported a mild pruritic sensation; however, most were asymptomatic. The trunk had the highest involvement frequency (89.7%), followed by the axillae and neck in both groups. Overall, the involvement of the flexural area, including the axillae and neck, was more common in the adolescent group (61.5%) than in the adult group (25%). Both extremities were rarely affected; only one patient had a lesion on the upper extremity, while no lower extremity involvement was observed in the adolescent group (Table 2, Fig. 1).
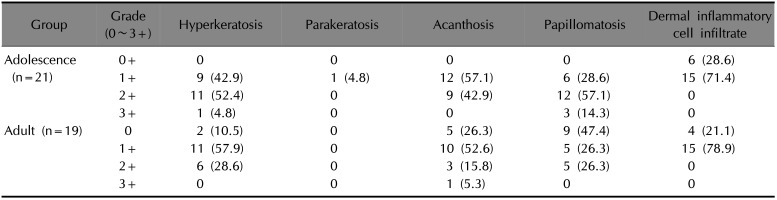
5) Histopathologic findings
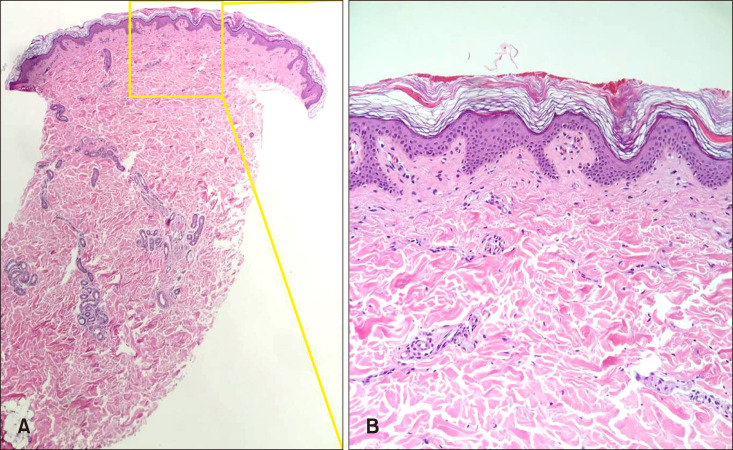
The pathologic findings did not show any significant differences but showed a slightly similar pattern. However, there was a difference between the age groups, which were analyzed on the basis of major histologic items, such as hyperkeratosis, parakeratosis, acanthosis, papillomatosis, and dermal inflammatory cell infiltrates (Table 3, Fig. 2). Hyperkeratosis of varying degrees was found in 38 specimens. Only one specimen showed severe hyperkeratosis, while the 37 specimens showed a mild to moderate grade. In the adolescent group, all 21 specimens showed hyperkeratosis, primarily mild (n=9, 42.9%) to moderate (n=11, 52.4%). In the adult group, mild (n=11, 57.9%) and moderate (n=6, 28.6%) hyperkeratosis were found. Parakeratosis was found in only one specimen (adolescent group).
Thirty-five specimens showed mild to moderate acanthosis. All specimens in the adolescent group showed mild to moderate acanthosis. Conversely, five of the adult patients showed no acanthosis, while the rest showed mild acanthosis. Papillomatosis was observed in 31 specimens. Three specimens had severe papillomatosis, whereas the remaining 28 showed mild to moderate papillomatosis. Papillomatosis revealed a distinctive pattern between the groups. In the adolescent group, all patients had moderate to severe papillomatosis; in the adult group, only 10 specimens (52.6%) showed mild to moderate papillomatosis.
A dermal inflammatory cell infiltrate was found in 75% of the 40 specimens. Most showed a mild degree of infiltrate, and there was no significant difference between the two groups.
DISCUSSION
The frequency of CRP internationally is unknown, and CRP is considered rare and is known to occur predominantly in young adults. In one study on 10 Lebanese cases2, half were of each sex, and the mean age at diagnosis was 19 years. In this study, the mean age was 19.3 years, which is similar to those of previous studies. CRP is not only rare but also poorly recognized by physicians, including dermatologists. Since Gougerot and Carteaud1 first identified CRP in 1927, this disease has been diagnosed on the basis of clinical courses, histologic findings, and treatment results. However, there have been misdiagnoses of CRP owing to a lack of diagnostic criteria for CRP. In a study on 39 patients, Davis et al.5 proposed the following criteria for the diagnosis of CRP (Gougerot–Carteaud syndrome): (i) clinical findings, including brown, scaly macules and patches, at least parts of which appear reticulated and papillomatous; (ii) involvement of the upper trunk and neck; (iii) negative fungal staining of the scales; (iv) no response to antifungal treatment; and (v) excellent response to minocycline. However, a few cases of CRP without trunk involvement have been described in the literature. The reported skin lesions were located in the popliteal fossa6, axilla67, or antecubital regions8. Those cases of CRP involved various flexural areas alone and fulfilled other diagnostic criteria for CRP. Jo et al.9 suggested the addition of revised diagnostic criteria to include flexural area involvement into the previous criteria5, which were limited to trunk and neck involvements.
In this study, two patients had a single lesion sparing the trunk: one in the axilla and one on the thigh (Table 1). Most of the patients had trunk lesions (89.7%), followed by axilla (27.6%) and neck (13.8%) lesions. Table 4 shows the clinical characteristics of the patients in this study in comparison with those in a previous study5. The demographics of the patients in the present study were in line with those in previous reports: CRP affects young adults. This disorder is thought to have no particular sex predilection; however, our study showed that the proportion of female patients was somewhat higher. It is uncertain whether this finding reflects its actual prevalence. Since CRP is almost asymptomatic, patients may visit the hospital seeking cosmetic improvement rather than symptom control. It also explains why the proportion of affected women was higher than that of men. Flexural area involvement, especially axillary lesions, was found in a larger number of patients in a previous study than in this study.
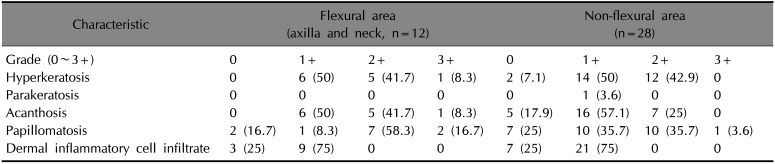
The histologic features in this study were similar to those reported in a previous study10. We found that the histologic changes were not associated with the disease duration. However, there were specific histologic changes in all patients by anatomic site. Table 5 shows the histologic features of the flexural (axilla and neck) and non-flexural areas. In the flexural area, half had high-grade (moderate to severe) hyperkeratosis, while most showed high-grade papillomatosis (75%); relatively mild hyperkeratosis and parakeratosis were seen in the non-flexural area. The acanthosis grades were similar, and it was confirmed that the flexural area had a more pronounced epidermal change than the non-flexural area. These findings were also related to the differences between the adolescent and adult groups (Table 3). The histologic changes in the epidermis were more significant in the adolescent group than in the adult group. Of the 40 total specimens, 19 were in the adult group (of which four were in the flexural area), whereas 21 were in the adolescent group (of which seven were in the flexural area). The reason for the more prominent histologic changes in the adolescent group might be that they had a greater flexural involvement. This is the reason why histologic changes of AN were found more commonly than those of CRP because AN is mainly present in the flexural area of the body11. As reported in many studies, patients with AN have associated malignancy12 and endocrine problems13; however, no such underlying disease was reported in patients with CRP in this study. Fungal infections appeared at a higher rate in the current study than in previous studies (Table 4). Of the 29 patients, five were no longer followed up, while the patients with fungal infections were treated with doxycycline and itraconazole. The rest of the patients were treated with doxycycline alone or combination therapy with phototherapy (narrow-band ultraviolet B), and their skin lesions improved thereafter. The 24 patients who completed the treatment were then examined to see how the treatment responses varied depending on their age, sex, and anatomic site. However, due to the small sample size within each treatment group, for which the same treatment was provided, assessment of treatment response could not be analyzed.
An additional study attempted to investigate whether there is a histologic difference according to erythematous-colored lesions and hyperpigmented lesions clinically seen in CRP; however, only six of the 29 patients had erythematous-colored CRP lesions. Therefore, it was difficult to obtain meaningful results owing to an insufficient number of samples.
There have been few studies regarding this condition on the Korean population, except for several case reports. In particular, an analysis of the association between age and anatomic site, as in this study, would aid in our understanding of the characteristics of CRP that have not yet been clarified.
The limitations of this study are as follows. First, the subject cohort was not large enough to enable further studies, such as determining sex-specific differences. Second, because the study had a retrospective design, there was a lack of multidisciplinary gathering of patient information, such as body weight, occupation, and previous skin problems, and many patients did not attend follow-up sessions to determine the treatment efficacy. Third, if the normal tissues of each patient were compared, individual differences might have been analyzed. In addition, histologic differences by body sites were not considered in this study. If large-scale and multicenter studies involving ethnic differences are conducted in the future, it will help us understand this disease better.
In conclusion, this study is the first to present the clinical and histologic features of CRP according to age and anatomic site in Korean patients. Skin lesions were seen at various sites, such as the neck, axillae, and bilateral extremities, in addition to the trunk. Histologic changes were more prominent in the adolescent group than in the adult group and in the flexural area than in the non-flexural area. The patients in this study more frequently had fungal infections (31%) than those in a previous study (12.8%).
 XML Download
XML Download