

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Kommerell's diverticulum is a rare congenital aortic anomaly accompanied by right side aortic arch and aberrant left subclavian artery (LSCA) arising from the diverticulum.1)2) This anomaly is a result of regression in the 4th left aortic arch between the left carotid and left subclavian arteries.3)4) This entity is usually detected incidentally on chest X-ray or barium esophagogram during the evaluation for the symptoms caused by the compression of trachea or esophagus by the diverticulum.5) We report the first case, to our knowledge, Kommerell's diverticulum initially detected by transesophageal echocardiography (TEE).
Case
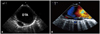
A 73-year-old, right-handed woman with a history of hypertension and diabetes was admitted to our emergency department with a suddenly developed aphasia. She initially had difficulty in expression but it resolved a few hours later. On admission, physical and neurological examination showed no abnormality except for the high systolic blood pressure (160 mmHg) and aphasia. Laboratory tests, including autoimmune markers and vasculitis serology, were normal. Electrocardiogram showed normal sinus rhythm with right bundle branch block. Brain magnetic resonance imaging with angiogram showed no evidence of cerebral infarction but bilateral internal carotid artery (ICA) stenosis. Based on the result of negative perfusion study, transient ischemic attack caused by artery-to-artery micro-embolism was highly suspected. So we performed TEE for the evaluation of cardiac source of embolism. TEE showed no definite source of emboli, evidence of shunt or aortic atheroma. During pull back, transverse view at the descending thoracic aorta (DTA) detected non-mobile bulbous echo-free space attached to the posterior aspect of DTA (Fig. 1A). Longitudinal view revealed that the space is connected to DTA and the Doppler study showed flow communication (Fig. 1B) suggesting that the space is outpouching vascular structure. Intimal flap, intimal rupture, spontaneous echo contrast or circumferential dilatation of DTA was not observed. Computed tomography (CT) angiogram showed right sided aortic arch with aberrant LSCA originating from the previously noted echo-free space on TEE (Fig. 2). Four-vessel angiography with aortography revealed mild to moderate stenosis of bilateral ICAs and aberrant LSCA arising from the aortic diverticulum (Fig. 3). The diagnosis was confirmed as Kommerell's diverticulum. But there was no evidence of esophageal or tracheal compression on the CT scan and she didn't complain any symptoms including dysphagia or hoarseness. The patient was discharged with 100 mg of acetylsalicylic acid and 75 mg of clopidogrel daily and been following up without any symptoms.
Discussion
Kommerell's diverticulum is usually discovered incidentally in asymptomatic adult patients, whereas some patients complain of severe symptoms caused by compression of adjacent organs by the diverticulum. Recently, TEE is frequently performed procedure in many purposes including not only for the embolic source evaluation but also for cardiac structure and hemodynamic evaluation. During the pull back period at the end of procedure, aorta should be evaluated for the existence of atheroma.5) When unusual space occupying structure other than the atheroma is observed, the possibility of other aortic diseases including aortic dissection, aortic aneurysm, pseudoaneurysm or tumor should be considered. In addition to these etiologies, the possibility of incidentally observed Kommerell's diverticulum and persistent left side superior vena cava (PLSVC) should be included in the differential diagnosis. When the structure is echo-free space out pouching from the DTA with a bulbous shape and blood flow connection exists, Kommerell's diverticulum can be considered and CT scan or magnetic resonance imaging is helpful for the exclusion of other aortic disease and confirmation of existence of right sided aortic arch and aberrant LSCA. PLSVC is the other type of congenital heart disease that can be observed during the TEE nearby the aortic arch similar with Kommerell's diverticulum. However, hypoechoic vascular structure of PLSVC on TEE can be differentiated with Kommerell's diverticulum showing respiratory variation and without pulsation. In conclusion, Kommerell's diverticulum can be detected on TEE in asymptomatic adult patients. So suspicion about this rare etiology on TEE can lead to further work up for accurate diagnosis and help clinician make decision earlier and the change the course of the disease.


 XML Download
XML Download