

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic Rhinitis (AR) is a common allergic disease that is defined as inflammation of the nasal mucosa. It is characterized by symptoms of rhinorrhea, sneezing, itching sensation, and nasal congestion.1 Clinical symptoms of AR are mainly triggered by inhalant allergens, of which the house dust mite is the most common aeroallergen in patients with respiratory allergy.23 The main treatment modalities for children who suffer from AR include medication and allergen avoidance.4 Although allergen avoidance is the core principle for successful therapy, complete avoidance is difficult to obtain for a house dust mite allergen in the environments of tropical countries.15
Nasal cellulose powder (NCP) has been approved as a remedy for AR.6 The NCP can react with moisture on the nasal mucous membrane, creating gel-like substance covering the nasal mucosa. This protective layer has been proposed to prevent an inhaled allergen from binding to receptors.7
Previous studies have suggested that NCP can reduce symptoms of persistent rhinitis from birch pollen allergy and dust mite allergy in adults.89101112 However, evidence for the efficacy of this product has not been provided in dust mite-sensitized AR children. The current study was conducted to determine the efficacy of NCP in improving clinical symptoms, nasal airflow limitations, and nasal inflammatory cell measures in dust mite-sensitized AR children.
MATERIALS AND METHODS
This randomized, double-blind, placebo-controlled trial was conducted at the Pediatric Allergy and Immunology Unit, Ramathibodi Hospital, Bangkok, Thailand between March and November of 2015. The study was reviewed and approved by the Human Rights and Ethic Committee of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand. All of the subjects or their parents provided written informed consent. This clinical trial was registered at Thai Clinical Trials Registry (No. TCTR20150325001).
Subjects
Children with AR aged between 6-18 years underwent the skin prick tested (SPT) and the nasal provocation test (NPT). Children who were positive to Der p allergen and had a history of AR symptoms for at least 1 year were enrolled. The exclusion criteria included: 1) manifestations of allergic symptom exacerbation, 2) other co-morbid allergic diseases, such as asthma, acute or chronic sinusitis, acute upper or lower respiratory tract infections, septal deformities, 3) multiple sensitization from SPT, 4) prior allergen immunotherapy, 5) current use of intranasal corticosteroids due to severe rhinitis symptoms.
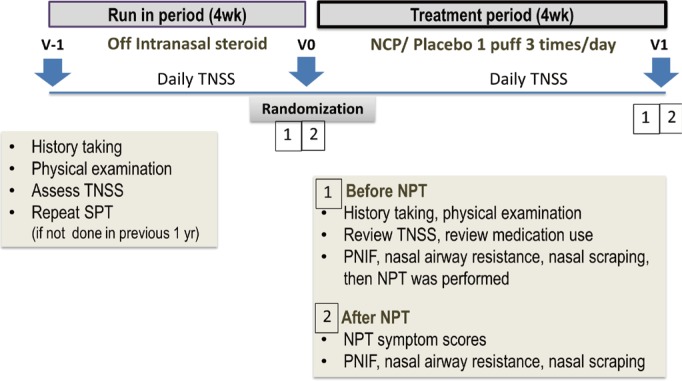
Baseline characteristics were recorded at screening. During a 4-week run-in treatment period, the children recorded their symptoms and use of rescue medications on daily diary record cards. The symptoms of nasal congestion, itching, rhinorrhea, and sneezing were all evaluated. The patients graded their symptom severity over the past 12 hours on a scale of 0-3: 0=absent, 1=mild, 2=moderate, and 3=severe.1314 The sum of these individual scores was referred to as a daily symptom score (DSS). The daily medication score (DMS) was calculated from the patient's daily diary record card on their use of rescue medications (oral anti-histamines and pseudoephedrine) and it was then noted on their daily diary record cards. Children were not permitted to use intranasal corticosteroids children during the experimental trial period. DMS was calculated based upon the magnitude and duration of clinical effect.1516 The daily combined score (DCS) was the sum of the DSS and DMS scores.15 The nasal airflow limitations (peak nasal inspiratory flow [PNIF] and nasal airway resistance [NAR]), as well as nasal eosinophil count, were evaluated at baseline and after treatment. The children were randomized to NCP (NoAl; Nasaleze International Ltd., Douglas, UK) or a placebo, with 1 puff each nostril 3 times daily for 4 weeks (Fig. 1). The placebo was lactose powder which had the same particle size and appearance as the NCP. This placebo was supplied in the same container. The containers were labeled with serial numbers. Both the patients and the investigators were blinded to these randomization codes. The randomization codes for NCP and the placebo were not revealed until all of the patients completed the study and all of the data were recorded. The medications, studied i.e., the NCP and the placebo, were supplied and supported by Nasaleze International Ltd. The participant's compliance with the treatment was assessed by using the medication daily record card. Text messages were sent 3 times a day to remind the subjects of taking take their study medication.
Nasal airflow limitation assessment
NAR was measured in each nostril separately by using active anterior rhinomanometry (Multifunctional Spirometer HI-801; Chest M.I., Inc., Tokyo, Japan). The PNIF was measured by using a nasal peak flow meter (In-Check Nasal; Clement Clarke, Harlow, UK).
NPT
The patients were asked to stop antihistamines and anti-leukotrienes for 1 week, oral ketotifen for 2 weeks, and oral or topical decongestants for 1 day before the NPT.17 The NPT protocols were as follows: first, baseline symptom scores were recorded, then anterior rhinomanometry was performed, and finally PNIF measured. To exclude any non-specific nasal hyper-reactivity, the patients were initially tested with a saline solution (0.9% NaCl). If the results of the saline solution NPT were negative, then the dust mite NPT was performed. A house dust mite (HDM) solution at different concentrations of the Der p allergen extract (50, 200, and 500 AU/mL) was applied to both nostrils at 15-minute intervals, in order to find the maximum tolerated dose. The total nasal symptom scores, the PNIF, and the NAR were assessed after each provocation. The NPTs were considered positive if one of the following criteria were met: 1) the NAR was increased by at least 20% of the baseline value, plus changes in the total nasal symptom scores from the baseline value by at least 3 points, 2) the NAR was increased by at least 40% of the baseline value, regardless of the total nasal symptom scores, and 3) PNIF was reduced by at least 20%.1819 After finishing the tests, the patients were asked to stay in the clinic for at least 30 minutes for clinical observation. Nasal irrigation, oral antihistamines, as well as oral decongestants, were given to patients with troublesome nasal symptoms.
Nasal scraping for nasal smear eosinophilia (NSE) grading
The nasal mucosal specimens were obtained by scraping the middle one-third of the inferior turbinate by using a Rhino-Probe™ Nasal Cytology Curette (ASI, Arlington, TX, USA) in both nasal cavities. The specimens were spread on microscope slides and then stained with Wright-Giemsa stain.20 The specimens were examined by using oil immersion under a light microscope and graded according to the NSE grading system.21 The same technician, who was blinded to the patient's identity and randomization, evaluated all of the specimens. For each slide, 5 randomly chosen magnification fields were examined and the eosinophil cell counts were recorded and graded on a 4-point scale.21
Statistical analysis
The randomization was provided centrally in a block of 4. Analysis was performed on all of the randomized patients who had both Visit0 and Visit1 follow-up data and had continued the study medication. A sample size of 28 patients (the treatment arm) was expected to have an 80% power to detect a difference of 9.4 between the NCP and placebo treatments in the mean total symptom scores from the nasal challenge,12 with a standard deviation (SD) of 12.2 and a 2-sided alpha error of 0.05. All statistical analyses were conducted using the SPSS 17.0 Software Package (IBM, Chicago, IL, USA). Nonparametric tests were used as follows: the χ2 test for the differences in the distributions of the actual frequencies of the scores; the Mann-Whitney U test for the medians and the correlations between the groups; and the Wilcoxon signed-rank test for the medians and the correlations within each group. A P value of <0.05 was considered to indicate statistical significance.
RESULTS
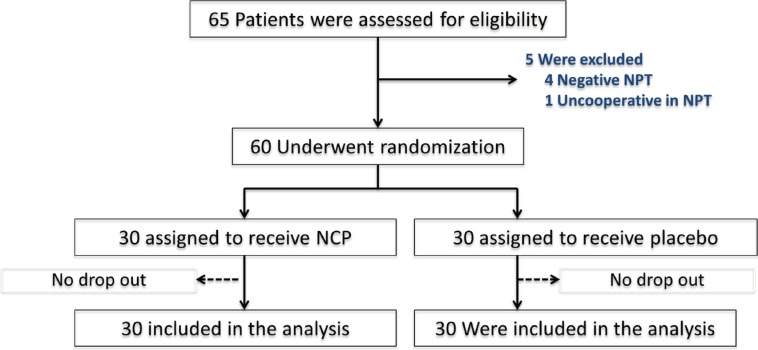
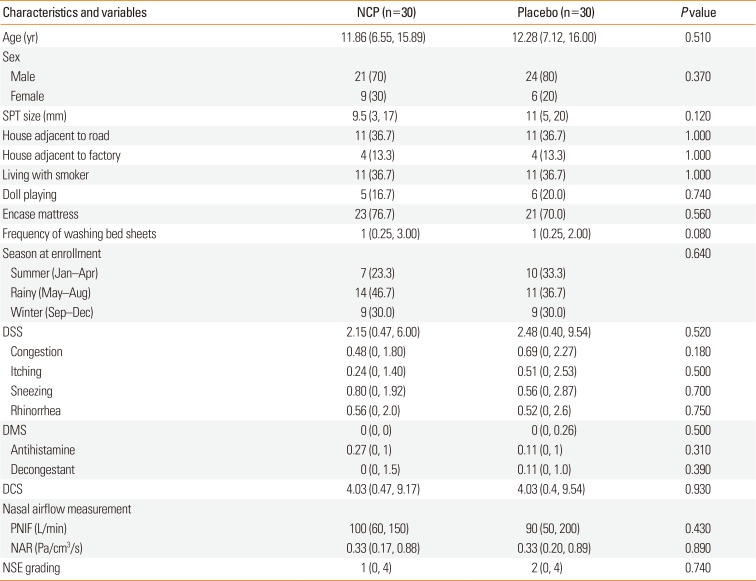
A total of 65 children with AR were screened and 60 children were randomized to 2 treatment modalities: NCP (n=30) and placebo (n=30). There was no patient discontinuation (Fig. 2). The mean age of the children was 11.6 years; 75 percent were male. The baseline demographic characteristics at entry were similar between the 2 treatment groups. There were no significant differences in the baseline values for the primary objective variables, including the DSS, DMS, PNIF, NAR, or NSE grading between the 2 groups (Table 1). The overall drug use compliance was 90.5%. There were no significant differences in the drug use compliance between the NCP and placebo groups (93% vs 88%, P=0.15). There were no systemic adverse reactions that occurred during the study.
Comparison between outcomes at baseline and after treatment
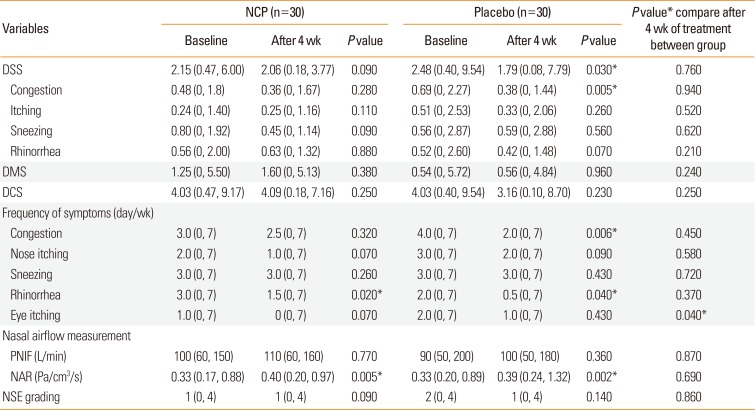
There was no significant difference between baseline and post-treatment DMS and DCS in either the NCP or placebo group. However, there was a significant decrease in the median DSS from baseline to posttreatment in the placebo group (2.48 [range: 0.40, 9.54] vs 1.79 [range: 0.08, 7.79], P=0.03). Children that received the placebo treatment had significantly lower median congestion scores when compared with the baseline scores (0.69 [range: 0, 2.27] vs 0.38 [range: 0, 1.44], P=0.005), but there were no significant differences in the DSS between baseline and post-treatment scores in the NCP group. Children in the placebo group had significantly lower median frequencies of congestion and rhinorrhea after treatment (4 [range: 0, 7] vs 2 [range: 0, 7], P=0.006) and (2 [range: 0, 7] vs 0.5 [range: 0, 7], P=0.04, respectively). While children in the NCP group had a significantly lower median frequency of rhinorrhea after treatment (3 [range: 0, 7] vs 1.5 [range: 0, 7], P=0.02). There was no significant difference in PNIF or NSE grade between baseline and posttreatment in either the NCP or the placebo group. Surprisingly, the NAR was significantly increased from the baseline values in both the NCP and placebo groups (0.33 [range: 0.17, 0.88] to 0.40 [range: 0.20, 0.97] Pa/cm3/s, P=0.005 and 0.33 [range: 0.20, 0.89] to 0.39 [range: 0.24, 1.32] Pa/cm3/s, P=0.002, respectively) (Table 2).
Comparison of outcomes between the NCP and placebo groups after treatment
There were no significant differences in the median values of DSS, DMS, DCS, PNIF, and NAR between the NCP and placebo groups after treatment. There were no significant differences in the NSE grade between the 2 treatment groups (Table 2). The changes in the maximal tolerated dose of NPT did not differ significantly between the NCP and placebo groups. Twenty-one patients in the 2 groups had positive NPT values at the same dose of Der p as before treatment.
Subgroup analysis
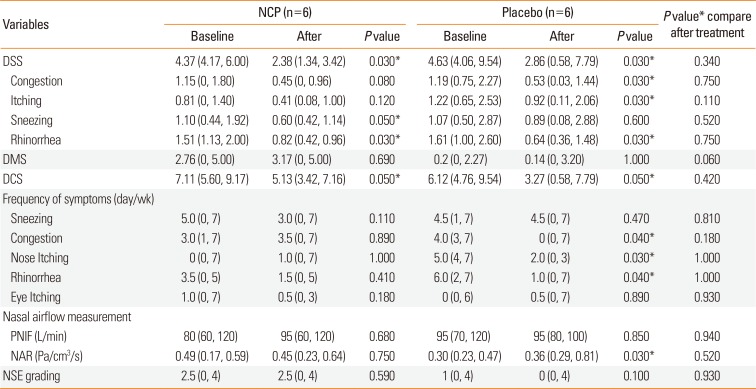
When conducting subgroup analysis for patients with moderate to severe symptom severity (in the DSS more than 4), significant improvements in the DSS and DCS from baseline were observed in both the NCP and placebo groups—DSS (4.37 [range: 4.17, 6.00] vs 2.38 [range: 1.34, 3.42], P=0.03 and 4.63 [range: 4.06, 9.54] vs 2.86 [range: 0.58, 7.79], P=0.03) and DCS (7.11 [range: 5.60, 9.17] vs 5.13 [range: 3.42, 7.16], P=0.05) and 6.12 [range: 4.76, 9.54] vs 3.27 [range: 0.58, 7.79], P=0.05). However, significant improvements in the frequencies of the symptoms of congestion, nose itching, and rhinorrhea were observed only in the placebo group (4 [range: 3, 7] vs 0 [range: 0, 7], P=0.04; 5 [range: 4, 7] vs 2 [range: 0, 3], P=0.03; and 6 [range: 2, 7] vs 1 [range: 0, 7], P=0.04), respectively. In addition, children who received the placebo treatment had a significant increase in NAR when compared with the baseline values. No significant differences were observed in either of the after treatment outcomes between the NCP and placebo groups (Table 3).
DISCUSSION
NCP was registered as a medical device for the treatment of AR. The current study has evaluated the efficacy of NCP in confirmed dust mite-sensitized AR. Our randomized, double-blind, placebo-controlled study has shown a similar efficacy of NCP and the placebo in clinical symptom scores, nasal eosinophil counts, and objective measurements of nasal airflow limitation. These results are in contrast to those of previous double-blind placebo-controlled studies, which have demonstrated the efficacy of NCP over the placebo treatment in patients with birch pollen AR, in terms of reductions in symptom scores811 and rescue medication use.9 These differences may be explained from the amount and presence of allergen exposure to AR patients. In tropical countries, such as Thailand, dust mite allergens are present all the year. This is in contrast to birth pollen which is a seasonal allergen. The amount of allergen has been shown to have an impact on the efficacy of NCP in children and adolescents suffering from birth pollen AR. The best efficacy of NCP has been demonstrated during low or moderate pollen counts.8 In the current study, we did not measure the levels of dust mite allergen in the environments of the enrolled children. The levels of dust mite antigen may have had an effect on the efficacy of NCP in dust mite-sensitized AR.
The Hawthorne effect22 is a social psychological change in the behavior of research participants as a response to the observations and the assessments which could possibly have had an impact on the clinical symptoms scores, as has been reported from our enrolled subjects. Since there was a similarity between the appearances of the NCP and the placebo, the treatment modalities were randomized and the patients were blinded to the treatment allocations. The Hawthorne effect would occur similarly in both groups. Previous studies have reported and proposed that the Hawthorne effect can be controlled by double blind-studies.23 Our investigation team and the patients were also blinded to the treatment allocations in order to minimize the Hawthorne effect.22
The severity of clinical symptoms of AR may have had an effect on the efficacy of NCP. However, several previous studies have evaluated the efficacy of NCP in patients who have stopped the use of intranasal steroids or have never used them before and during the enrollment,8911 which is similar to our study. A recent study has demonstrated the efficacy of NCP in enhancing oxymetazoline-increased PNIF in adults with moderate to severe persistent perineal AR.24 A real-life study on the effects of NCP as an add-on to intranasal as-needed treatment, in subjects with pollen AR has demonstrated a decrease in combined symptom and medication scores (CSMS) in patients receiving NCP when compared to those receiving placebos.25 Further studies on the efficacy of NCP as add-on treatment to intranasal steroids are needed to demonstrate the efficacy of NCP in patients with moderate to severe persistent perennial AR.
The efficacy of NCP in preventing allergic symptoms after a dust mite challenge has been demonstrated in a small randomized controlled trial with adults using 2 puffs of NCP per nostril before the NPT with Der p1 and Dermatophagoides farina (Der f1).12 It has been shown that patients had less rhinorrhea/sneezing and better PNIF in the NCP group than in the placebo group.12 Nevertheless, the current study has demonstrated that treatment with NCP at 1 puff per nostril 3 times a day for 4 weeks did not improve the nasal symptom scores, PNIF, NAR, or NSE grades, more than treatment with the placebo. One apparent difference from a previous study is that the dosage of NCP was lower. However, the dosage of 1 puff per nostril 3 times a day is the recommended dosage from the manufacturer. In addition, this dosage and 4 weeks of treatment have been shown to have an efficacy in reducing AR symptoms in seasonal AR.81112 Higher doses of NCP may need to be studied in order to evaluate the efficacy of NCP in dust mite-sensitized AR patients.
The strength of the current study is that all of the enrolled patients were confirmed to have AR symptoms due to dust mites by performing dust mite nasal challenge tests. We have also evaluated objective measurements of nasal obstruction (PNIF and nasal resistance), clinical nasal symptoms scores, medication scores, and nasal eosinophil counts. The limitations of the current study were as follows. A daily diary record card could improve patient compliance with the studied drug when only using. The nasal powders were supplied in a plastic container which delivered the powder from a nozzle when squeezed. The exact amounts of the delivered powder were not standardized and the patterns of its a deposition in the nose are not well studied.8 As a result, the exact amounts of the studied drug when entering the nose of the enrolled patients could not be correctly measured. Nasal symptom scores were evaluated by the self-reported scoring questionnaire filled out by the patients. Inherent biases from the patient's feelings at the time they filled out in the score may occur. However, this effect would have a minimal impact on the results of our study. Since, both the patients and the investigators were blinded to the medication assignment, the medication assignment was randomized and the objective measurement of nasal obstruction were also possible. Furthermore, the dust mite levels in the environment were not measured. The levels of the dust mite antigen may have had an effect on the efficacy of NCP in dust mite-sensitized AR children.
To our knowledge, this is the first study that has evaluated the efficacy of NCP in dust mite-sensitized AR children. We have shown that NCP treatment at 1 puff per nostril 3 times a day for 4 weeks has had a similar effect to the placebo treatment. Further studies are needed to validate the efficacy of NCP in dust mite-sensitized AR children.
 XML Download
XML Download