

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic diseases, hypersensitivity disorders of the immune system, are a major global health concern. Pediatric allergic diseases comprise a large component of general pediatric care and are increasing in prevalence.1 The phenotype of allergic diseases tends to transform from atopic dermatitis to allergic rhinitis and asthma, and threaten the quality of life of affected children and their parents.
During pregnancy, women are more vulnerable to stress and at risk of distress due to profound hormonal and physiologic changes. Prenatal maternal distress is thought to influence various fetal and neonatal outcomes: prematurity and intrauterine growth restriction, psychiatric diseases, and the metabolic syndrome.2 Given the high prevalence of prenatal maternal distress and substantial medical burden of allergic diseases, investigation of the association between prenatal maternal distress and allergic diseases in offspring, and the possible underlying mechanisms, warrants attention.
In this review, we aim to summarize current evidence on the impact of prenatal maternal psychological distress on the development of allergic diseases and to discuss possible pathways linking prenatal stress and allergic diseases. Through this, we will present a viewpoint of selecting vulnerable subgroups and choosing intervention strategies.
EVIDENCE OF THE IMPACT OF PRENATAL MATERNAL DISTRESS ON ALLERGIC DISEASES IN THEIR OFFSPRING
To locate current evidence on the topic, we conducted a keyword search through the PubMed databases (see Supplementary Table available from http://www.e-aair.org). From the 238 results, we selected cohort or registry studies published between January 1, 2000 and June 30, 2016 that examined the association between prenatal maternal distress and allergic diseases in offspring. We chose original articles where the primary exposure involved prenatal maternal psychological stress, and the main outcome covered any allergic disorder (wheezing, asthma, allergic rhinitis, atopic dermatitis, atopic eczema, allergic conjunctivitis, or food allergy).
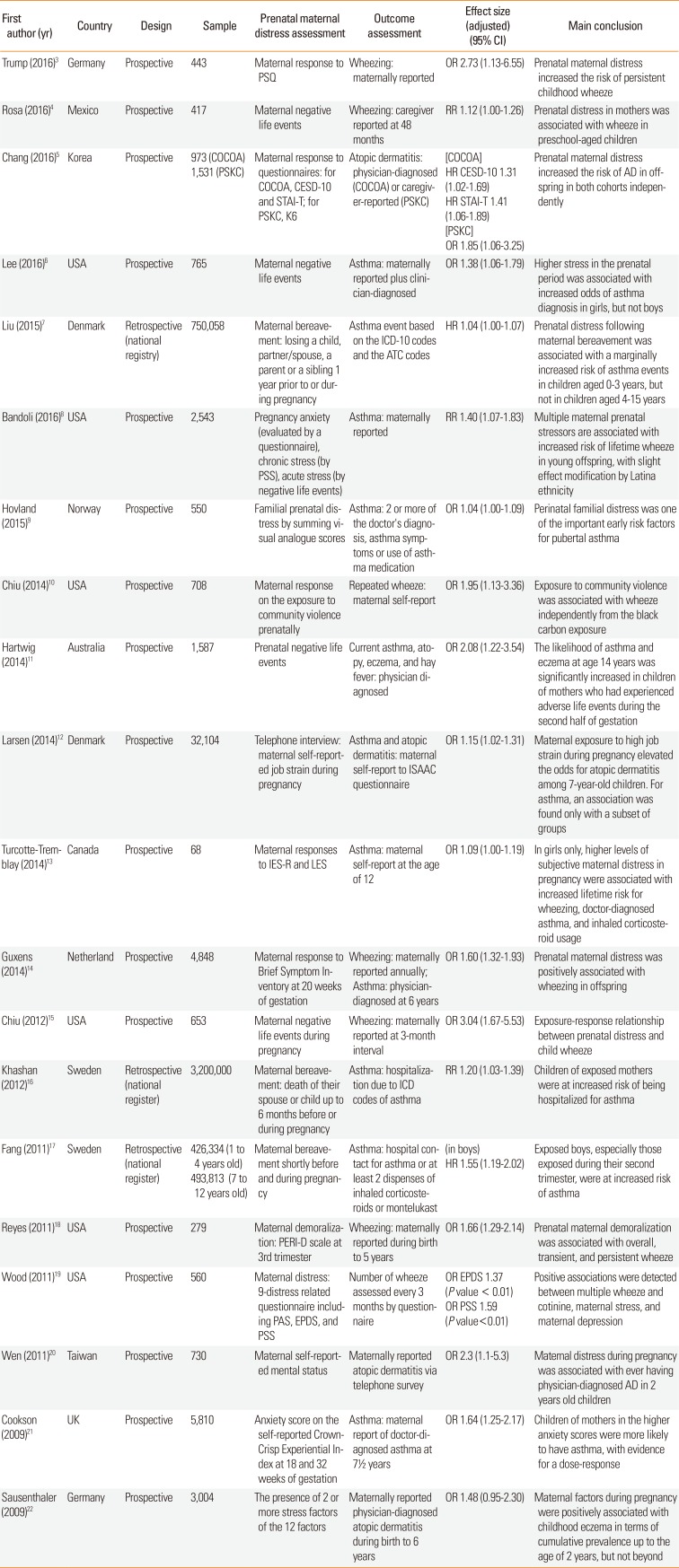
Table summarizes the selected published studies. A total of 20 studies were chosen:345678910111213141516171819202122 17 prospective cohort studies 3456891011121314151819202122 and 3 national registry studies.71617 Most studies used general population samples, although not all were nationally representative. Prenatal maternal distress had a close association with wheezing/asthma in 17 studies346789101112131415161718192122 and atopic dermatitis in 5 studies.511122022 Two studies reported good relationships with both asthma and atopic dermatitis.1122 Only 1 cohort study assessed the possible relationship between maternal distress and allergic rhinitis.11 The earliest report on the effect of prenatal maternal distress on allergic diseases was published only in 2009,2122 which may be related to the fact that the fetal origins hypothesis began gaining substantial attention during the late 1990s and the International Society for Developmental Origins of Health and Disease was established in 2003. Although we have not proceeded a meta-analysis, the attributable risk of prenatal maternal stress seems to be present but limited. Although these are lists of studies that presented only positive results, 16 out of 20 (80%) studies presented odds, relative risk, or hazard ratio of less than 2. Moreover, no study has found a significant association between prenatal maternal stress and allergic rhinitis development.
Prenatal maternal distress was ascertained by various methods during different time periods. Regarding assessment points, studies using negative life events encompassed the whole pregnancy period,467811151617 while those using self-reported questionnaires on depression or anxiety were conducted during the second or third trimester. All but one study assessed maternal distress at just 1-time point, thus making it difficult to ascertain the critical period for the effect of prenatal maternal distress on fetal and neonatal immune development. A study conducted in the UK assessed prenatal anxiety at 2 time points, 18 and 32 weeks of gestation, and found similar trends of a positive association between prenatal anxiety and subsequent childhood asthma at 7½ years, though the estimated parameter was larger for anxiety during the third trimester.21
In some studies, negative or stressful life events were used as a proxy for prenatal maternal distress.4681115 Maternal bereavement involving a spouse or child, one of the most extreme traumas a person may face, was found to be significantly associated with later allergic diseases,71617 and the number of stressful life events during pregnancy was also reported to show a dose-response relationship.6 Recently, studies using validated self-reported questionnaires have also been published.3581314181921 However, there are as yet no studies that applied observational or objective measures to assess maternal psychological status. While there is evidence that maternal distress during pregnancy is associated with cortisol disruption,23 the relationship between cortisol dysregulation and its effect on the fetus is yet to be examined.
Regarding the outcomes, most studies used maternal reports on their child's allergic symptoms. However, it is possible that mother's recognition and reporting of the child's symptoms may be affected by their psychological status, since depression or anxiety is known to color perception.24 Two studies in Sweden utilized hospital records to assess the presence of asthma in a large representative general population sample.1617 While hospital records provide comparatively more objective information on the medical status of subjects, registry studies are limited by potential residual confounding due to factors not recorded in the register. One study used physician's diagnosis of allergic diseases based on symptoms reported by mothers and children to ascertain asthma,14 with no objective measurement, such as pulmonary function or bronchial provocation testing.
In summary, there are several points to note in designing or interpreting studies involving the relationship between prenatal distress and allergy diseases. First, prospective data is crucial to examineing the association between more delicate psychological status and later development of illness, since symptoms like depression or anxiety are more prone to become biased. For fear of a recall bias, the retrospective approach should be confined to certain life events, such as the death of a spouse. Secondly, ascertainment of allergic diseases based on the maternal reports may be easily biased since mood states are known to influence the perception of current allergic illnesses.24 Mothers who are depressed or anxious may be more vigilant to minimal changes in the child, which may result in the overestimation of outcome diseases. Thirdly, the definitions of prenatal distress are variable: some studies measured 1 or 2 major life events, such as bereavements or the number of stressful life events, while others used validated questionnaires. Finally, most of the studies did not adjust for potential confounders, such as other risk factors for allergic diseases and postnatal maternal distress.
These studies demonstrate that there is sufficient evidence to conclude that prenatal maternal distress is associated with later development of offspring's allergic diseases. Most studies are, however, focused on asthma/wheezing; hence, there is a need for publications concerning other allergic diseases, such as allergic rhinitis or food allergy.
POSSIBLE PATHWAYS LINKING PRENATAL MATERNAL DISTRESS AND ALLERGIC DISEASES
Psychological stress is known to exacerbate allergic diseases via endocrine or immune responses.25 Considering that atopy is related to dysregulated immunity and that exposure to any risk factors during the critical period of development can affect the immune system's maturation, psychological stress during the fetal period may play a role in the onset of allergic diseases. However, few reports have postulated mechanisms by which prenatal maternal distress affects allergic diseases in offspring.
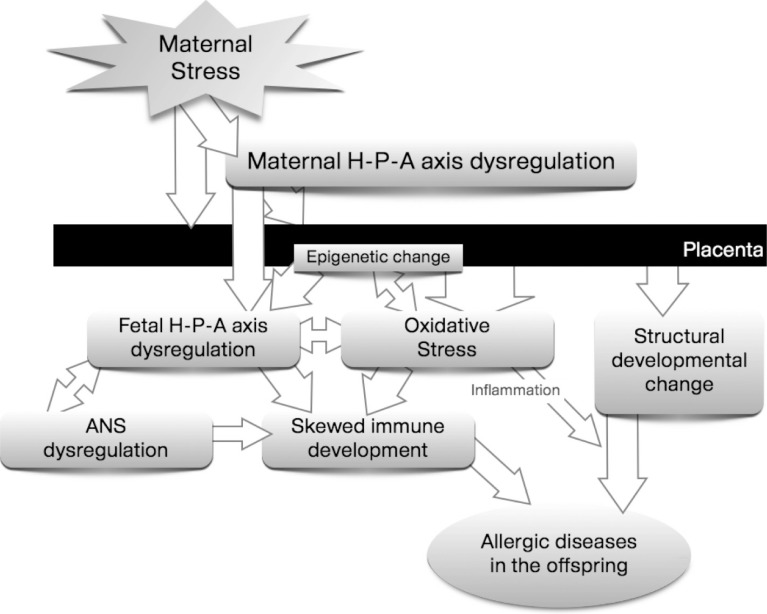
Since fetal and perinatal periods are the most critical phases of development, the risk of atopic disorders may mainly be ascribed to perinatal programming, and contributed to by non-genetic and environmental factors.26 Psychological stress is one of the suspected key factors playing a role in programming.2 In response to distress, the homeostatic regulatory system acts to maintain the body's equilibrium. This is necessary as a short-term response to stress, but may produce damage in the long-term.27 If not checked and eventually terminated, the stress response might permanently alter the responsiveness of major regulatory systems with serious impacts on the developing immune system and, consequently, may enhance the risk of diseases. It will be helpful to review the possible mechanism in terms of 5 aspects, in order to understand the whole process linking prenatal distress and allergic diseases in offspring collectively (Figure), as discussed below.
Psycho-neuro-endocrine dysregulation
The hypothalamic-pituitary-adrenal (HPA) axis and autonomic nervous system (ANS) are key regulatory systems activated in neuroendocrine pathways in response to environmental stress. The offspring's HPA axis or ANS, when persistently activated, can push the offspring's immune development toward being allergy-prone. This is a suspected mechanism of the maternal stress-induced development of asthma and allergic diseases in offspring.2829 Since psycho-neuro-endocrine systems are interrelated, it may be difficult to separate the effect of each pathway, and altered neuroendocrine or autonomic systems can induce dysregulation of other systems. Any physical or psychological stress that can affect fetal psycho-neuro-endocrine systems could cause offspring's allergic diseases.2628
A dysregulated HPA axis is one of the representative pathophysiologies in this relationship.
Chronic stress may alter the maternal HPA axis.230 Pregnant women experiencing much distress have persistently high levels of cortisol.31 Elevated levels of maternal serum cortisol result in more cortisol passing through the placental barrier, thereby increasing the cortisol level in the fetus.30 Maternal cortisol can also stimulate production of placental cortisol-releasing hormone (CRH) leading to elevated fetal CRH levels.228 Moreover, maternal distress itself reduces uteroplacental blood flow initiating a fetal stress response with subsequent fetal HPA axis activation.32 These all may eventually alter the responsiveness of the fetal HPA axis. Persistently elevated fetal CRH and glucocorticoid levels can influence brain and central nervous system (CNS) development, leading to long-term changes in HPA axis regulation, which in turn predisposes to later expression of asthma and allergic diseases.25
Alterations in the ANS, along with a dysregulated HPA axis, may polarize the fetal immune system toward allergic diseases. Maternal psychological stress activates the fetal sympathetic adrenomedullary system as well as the HPA axis.28 Furthermore, catecholamines increase the level of glucocorticoids, which in turn affects the HPA axis. ANS activation affects the immunologic system, possibly in a bidirectional way. This is called the neural-immune response.29 Vagal output regulates peripheral immune responses by suppressing the innate immune defense to pathogens and by altering the balance of pro-inflammatory cytokines.2833 On the other hand, local immune activation elevates pro-inflammatory molecular mediators, which not only influence cells of the innate/adaptive immune system in the periphery but also activate sensory pathways that relay information to the CNS.29 In asthma, cholinergic vagal systems are deeply engaged in the pathophysiology. Inflammation damages the m2-autoreceptors which in health downregulate cholinergic transmission at the level of the postganglionic nerve terminal, thereby limiting the constriction of airway smooth muscles.34 Animal studies have demonstrated that the neural control of airway smooth muscle function and irritant receptor systems are established during the perinatal period.
The ANS can also influence atopic sensitization and the expression of allergic disorders via neurotransmitters. Some neurotrophins are thought to be mediators or moderators of allergic diseases, and their expression and signaling may be influenced by stress: brain-derived neurotrophic factor, tumor necrosis factor-alpha, and tachykinin-like substance P were suggested in an animal and human study.28
Concerning the programming of the ANS response, the role of catecholamines circulating at a high level in maternal blood is also worth focusing on. High levels of circulating catecholamines can alter placental or fetal 11β-hydroxysteroid dehydrogenase type II (HSD2) levels and activity, nutrient transport, and glucocorticoid receptor (GR) density, which may link maternal distress and fetal ANS alteration.2829
Altered placental function
The placenta is a major organ; it delivers maternal oxygen and nutrition to the fetus. In a stressed mother, blood flow to the placenta commonly decreases. Insufficient oxygen and nutrition can activate the fetal hormonal system and ANS, which may increase production of reactive oxygen species (ROS).3536 The placenta also moderates fetal exposure to maternal factors. 30 In a healthy pregnancy, glucocorticoids can pass freely across the placenta, but placental HSD2 provides a functional protective barrier between the fetus and mother. By converting active cortisol to inactive cortisone, HSD2 shields the glucocorticoid-sensitive tissues in the fetus from exposure to excessive glucocorticoid levels during development. Maternal distress, on the other hand, can down-regulate HSD2 activity. As maternal glucocorticoid levels are significantly higher than those of the fetus, subtle changes in HSD2 activity, including ones induced by maternal distress, can allow significant fetal exposure to excessive concentrations of glucocorticoids.2530
Maternal and fetal distress also stimulate CRH secretion in the placenta, which results in increased levels of CRH in the fetal circulation. This excessive fetal CRH can overstimulate the fetal HPA axis and amplify the state of fetal glucocorticoid excess and activating additional elements of the fetal stress response, influencing the ANS and immune system development.2830
Oxidative stress and epigenetic changes
ROS denotes a number of reactive molecules and free radicals derived from molecular oxygen, such as hydrogen peroxide, superoxide ions, hydroxide radicals, and nitric oxide. During normal cellular activities, various processes within the cells produce ROS. ROS take part in host cell defense mechanisms via radical formation and also play a role in cell signaling, including apoptosis, gene expression, and the activation of cell signaling cascades.37
Oxidative stress, on the other hand, refers to an imbalance favoring the pro-oxidative state, i.e., production of ROS exceeds the removal of ROS.36 Pregnancy is one of the typical physiological conditions associated with oxidative stress. A high metabolic turnover and elevated tissue oxygen requirements increase oxidative stress. Markers of oxidative stress rise in the serum even during a normal pregnancy.36 Newborns exhibit an accelerated production of free radicals and have limited antioxidant protection, making them highly vulnerable to oxidative stress. Therefore, any maternal condition that may induce oxygen-radical overproduction, such as hypoxia, inflammation, or infection, 37 can result in a state in which the capacity of defensive mechanisms to neutralize them may be exceeded and may augment the detrimental impacts of oxidative stress on the fetus.
Maternal psychological stress can increase oxygen requirements and may place the fetus under more oxidative stress during pregnancy. The higher levels of glucocorticoid induced by distress can inhibit glucose utilization and compromise the activity of energy-dependent excitatory amino acid transporters, which may increase intracellular Ca2+ concentrations and activate Ca2+-dependent enzymes. As a result, these processes can activate production of ROS. In addition, compromised mitochondrial respiration contributes further to ROS production.37
Recently, for the first time, researchers using a Korean birth cohort study have succeeded in demonstrating clues for a series of pathways involving prenatal psychological distress, HPA axis dysregulation, and elevated oxidative stress.5 They measured placental HSD2 levels directly from a subgroup of the cohort sample and found that children without either allergic diseases or prenatally distressed mothers had significantly higher placental HSD2 levels than those with prenatally distressed mothers, regardless of their later allergic disease development. Moreover, they assessed the glutathione to glutathione disulfide (GSH/GSSG) ratio—a marker for oxidative stress—directly from the placenta and found that the GSH/GSSG ratio was lower in mothers who were distressed than in those who were not.
Findings suggest that oxidative stress can induce an atopic condition which is perpetuated by the activation of oxidative stress-related genes.36 Oxidative stress could influence T-cell signal transduction and gene expression, and modulate T-cell polarization toward a T helper 2 (Th2) cellular subset, which might, in turn, be a further source of ROS. Furthermore, oxidative stress can alter the physiologic functioning of the HPA axis, induce damage in keratinocytes, and facilitate the release of cytokines in the airway. These observations collectively suggest that oxidative stress induced by prenatal distress may play some role in the pathogenesis of offspring's allergic diseases.
On the other hand, epigenetic dysregulation of gene expression has recently drawn attention as a potential mechanism for developmental programming.236 Not only the genetic code but also the epigenetic modification (i.e., DNA methylation, histone modification, regulatory RNA molecules) can affect gene expression and regulation.38 Since plasticity is the main feature of fetal and early infant development, long-lasting changes in gene expression, i.e., transcriptional repression during a critical period, may cause adverse outcomes in the offspring.27 DNA hypermethylation and specific histone residue hypoacetylation are reported to be involved in the pathogenesis of asthma and other allergic diseases. The methylation of anti-inflammatory genes (i.e., the runt-related transcription factor 3 [Runx3]) and the methylation of CpG islands covering the promoter and exon 1 region of the HSD11B2 gene raise the risk for allergy development. Also, exposures that inhibit histone deacetylases (i.e., oxidative stress) enhance NFkB driven transcription of inflammatory genes, and up-regulate Th2 cytokine (interleukin [IL]-13, IL-5) and GATA3-mediated T cell responses, which may induce characteristic features of asthma and allergic diseases.3839
Several studies have reported the association between prenatal maternal distress and epigenetic changes in the region that increases allergy risk. Increased methylation of the NR3C1 promoter40 and decreased methylation of the SLC6A4 promoter41 are found in the cord blood of newborns born to stressful mothers. Prenatal distress also influences methylation in the corticotrophin releasing factor promoter and GR promoter regions of the hypothalamus as well as in the HSD11B2 promoter region within the placenta, controlling excessive glucocorticoid exposure to the fetus.42 Due to the rapid development of laboratory technology, a recent study has succeeded in demonstrating direct links between maternal distress, epigenetic changes, and the development of allergic diseases. They studied differential DNA methylation at the time of birth by whole genome bisulfite sequencing of 10 mother-child-pairs, which is complemented by longitudinal targeted methylation and transcriptional analysis in over 300 children registered in a birth cohort.3
Skewed immune development
Programming of the immune system, a skewed immune development prone to allergic disorders, comprises the later part of the mechanism by which maternal distress affects offspring's allergic sensitization and risk of allergic diseases. Evidence shows that maternal distress can affect offspring's immune system in various ways. First, maternal distress directly changes the immune system. Innate immunity is compromised by maternal distress.29 Maternal distress limits macrophage and neutrophil function, and attenuates natural killer cell cytotoxicity.43 By resetting homeostatic set points and the responsiveness of stress pathways, maternal distress can change the pattern of macrophage-derived cytokine release and, consequently, may adjust the regulatory mechanisms related to spreading and phagocytosis. Acquired immunity can also be affected by maternal distress.29 The size, morphology, and function of the thymus may already be altered at birth.43 In an animal study, the number of total peripheral blood lymphocytes and the numbers of CD4+ and CD8+ lymphocytes decreased in offspring whose mothers were stressed. Lymphocyte responses to mitogens decreased, but to varying degrees depending on the age and sex of the offspring and the specific mitogen. Maternal distress can also affect passive immunity2943 by modifying the ability to transfer maternal immunoglobulin G (IgG) to the offspring in utero. Reduced circulating serum IgG levels have been observed in offspring after psychological stress during the third trimester of pregnancy, the time of active transplacental transfer of maternal IgG.
Maternal distress modulates physiological systems that regulate the immune system.2829 It stimulates the fetal HPA axis to amplify fetal glucocorticoid production and activates additional elements of the fetal stress response, i.e., catecholamine release. Glucocorticoid levels are elevated by stress trigger apoptosis of all thymocyte subpopulations, especially immature CD8+ cells that are highly sensitive to glucocorticoids. Moreover, glucocorticoids inhibit the production of IL-12 and interferon-γ by antigen presenting cells and Th1 cells, upregulate the production of IL-4, IL-10, and IL-13 by Th2 cells, and prevent the development of regulatory T (Treg) cells.282938 These all may induce selective suppression of Th1-mediated cellular immunity and trigger a shift toward Th2-mediated humoral immunity.
Finally, prenatal maternal distress can also affect central autonomic sites with or without altering the innervation of target tissues that are essential for immune modulation.28 The sympathetic nervous system regulates the balance of Th1 and Th2 in the uterus to influence the implantation and development of embryos during early pregnancy. Based on animal study results, sympathetic denervation is thought to up-regulate T-lymphocyte numbers and change cytokine levels in the uterus, altering its immune environment.
Structural developmental changes
Structural changes other than inflammation have also been noticed in asthma and allergic diseases. In asthma, structural alterations in small airways drive the airway physiology so as to promote airway narrowing, hyperresponsiveness, and inflammation.42 In atopic dermatitis, dysfunction in the epidermis, especially in the stratum corneum, results in defective epidermal permeability and a propensity to secondary infection.36
Concerning asthma, glucocorticoids play a significant role in regulating fetal and postnatal lung development.42 Fetal and early postnatal exposure to endogenous or exogenous corticosteroids attenuates lung development, and these structural alterations persist. Moreover, a high level of fetal glucocorticoids is itself related to preterm delivery or low birth weight, which may potentiate the later development of asthma and allergic diseases. In subjects from stressed mothers, oxidants can react with all cellular macromolecules, particularly polyunsaturated fatty acids on the cell membrane. Thereafter, a chain reaction is started, proceeding to cell injury and, ultimately, cell death. Oxidative stress also promotes tissue inflammation through up-regulation of genes that encode proinflammatory cytokines.37 All these processes may damage keratinocytes and increase the risk of atopic dermatitis.44
Interaction with other potential confounders
Fetal exposure to various environmental factors is also thought to influence the development of allergic diseases later in life,26 which can explain why we fail to estimate an individual's risk for developing later allergic diseases merely based on maternal distress exposure. These factors are thought to modulate the allergic manifestations independently of, or via indirect interaction with, prenatal distress.
First, familial factors, such as parental history of atopic diseases, are associated with an increased risk of atopic diseases in offspring.45 Although no reports are available on whether parental atopy plays a synergistic or antagonistic role with prenatal distress in developing allergic diseases, the effect of prenatal distress is enhanced in the absence of a maternal atopic predisposition. 11 Sex difference can also modulate the risk of allergy development in offspring. In general, childhood asthma is more common in boys. Sex-specific differences have also been reported for bronchial hyperresponsiveness, allergic sensitization, serum immunoglobulin E (IgE) levels, and the developmental cytokine response profiles.46 In a study using data from the Lifestyle and environmental factors and their Influence on Newborns Allergy risk cohort, the risk for allergic diseases at 1 year increased in boys and was associated with fewer Treg cells in their cord blood specimens.47 Sex differences can modulate the impact of other factors on asthma risk via the genotype-by-sex interaction. Moreover, the effect of prenatal distress on HPA function is substantially more marked in girls than in boys.48 Secondly, physical factors, such as intrauterine growth restriction, are also closely associated with prenatal distress,49 possibly through uteroplacental insufficiency and maternal unhealthy habits, including poor sleep pattern, sedentary lifestyle, or a greater propensity for alcohol abuse and cigarette smoking. Moreover, intrauterine growth restriction in itself can affect the development of asthma.26 Thirdly, in utero exposure to indoor pollutants, such as environmental tobacco smoke (ETS), independently influences fetal lung development and uteroplacental flow,50 thus increasing the risk of asthma in offspring. Moreover, in a study, fetal exposure to ETS decreased the number of Treg cells, which was associated with elevated risk for offspring's allergic diseases.51 Both ETS and prenatal maternal distress can augment oxidative toxicity and airway inflammation in offspring,5253 which may predispose offspring to an allergic airway disease. Fourthly, exposure to outdoor pollutants is itself closely associated with the intermediate phenotype of asthma. In children, air pollution interacts with past episodes of bronchiolitis in the development of asthma.54 Moreover, exposure to traffic exhaust particles increases oxidative stress and has epigenetic effects during pregnancy.55 In a study, exposure to particulate matter with a diameter of less than 2.5 µm (PM2.5) during pregnancy was associated with increases in wheezing during early life. Moreover, when combined with exposure to community violence during fetal periods, the risk of wheezing is greater in infants with exposure to PM2.5 or black carbon.10
Finally, postnatal maternal distress may impact the early childhood environment and caregiving experience, which may change the development of stress reactivity in children and, in turn, can influence the occurrence and persistence of allergic diseases.56 According to a birth cohort study, parental distress is a predictor of wheezing in infancy and chronic caregiver stress is associated with dysregulation of immune function.57 On the other hand, a child's psychosocial stress may also operate as a moderating factor. Allergic and psychological problems have a tendency to co-occur, and, according to a meta-analysis, a bidirectional relationship is found between mental health symptoms and atopic disorders.58 Moreover, children with depressive or anxious temperaments are at risk of asthma and other allergic diseases.59
We conclude that prenatal maternal distress may affect fetal programming to allergic diseases directly or indirectly. Both dysregulation of the HPA axis and increased oxidative stress may cause structural (altered brain/lung development) or functional (skewed immune system development) changes, which may predispose the fetus to develop allergic diseases during childhood. Although many facts are yet to be discovered, changes in placental responses and epigenetic modifications are presumed to mediate the process from maternal distress to allergic diseases.
FUTURE PERSPECTIVES
Challenging role of gut microbiome: the most potent modulator in the prenatal distress-allergic disease association
The gut-brain axis links emotional and cognitive centers of the brain with peripheral intestinal functions. Since the central and enteric nervous systems communicate bidirectionally, psychological problems or stress can affect functional bowel disorders, and vice versa. Neuro-immuno-endocrine mechanisms mediate the bidirectional communication network that includes the CNS (both brain and spinal cord), ANS, enteric nervous system, and HPA axis.60 Recent advances in research have demonstrated that the gut microbiota plays an important role in modulating these interactions. This interaction between microbiota and gut-brain axis appears to be bidirectional, namely through signaling from gut microbiota to the brain and from the brain to gut microbiota, which is called the Microbiota-Gut-Brain (MGB) axis.61 In germ-free animals, introduction of and changes in microbiota are shown to modulate an anxiety-related behavior against stress testing.62 Moreover, fecal microbiota transplantation is now used to treat autism, attention-deficit hyperactivity disorder, multiple sclerosis, and chronic fatigue syndrome61 as well as inflammatory bowel diseases, metabolic syndrome, and obesity. Possible mechanisms include Treg cell induction through probiotic-related innate immunity activation. 63 Moreover, the MGB axis involves neural, endocrine, immune, and humoral mediators; hence, it may be inferred that the MGB axis can modulate the pathogenesis of allergic diseases. 63 In an experimental food allergy model, microbial signatures determined allergic sensitization and anaphylaxis.64 At a human level, the hygiene hypothesis initially introduced by Strachan to explain the allergic epidemic, is now re-interpreted as changes to the gut microbiome that are crucial to normal immune development or the pathogenesis of allergy.65 Even probiotics are now appraised for their role in preventing or modulating allergic diseases.63 Furthermore, there is indirect evidence of the involvement of microbiota in the pathogenesis of the prenatal distress-induced offspring's allergy. The microbiome affects psycho-neuro-endocrine dysregulation, oxidative stress and epigenetic regulation, skewed immune development concerning the increased inflammation and lack of tolerance induction as well as the allergy-prone deviation in T-cell response, physical growth, and development, moderating responses to pollutants, and psychological problems in early childhood.63 Nevertheless, few studies have clearly demonstrated the role of microbiota in modulating the association between prenatal distress and the development of allergic diseases. This should be explored as it offers a promising target for secondary intervention.
Possible biomarkers to identify highly susceptible subgroups
A few years ago, when the epidemiologic association was not verified, researchers focused only on building a prospective birth cohort. Hence, they did not gather sufficient prenatal or perinatal biologic samples related to prenatal exposure or immunologic changes. Moreover, the lack of information on potential confounders still limits the interpretation of marginal associations. As a result, despite the clear association between prenatal distress and offspring's allergic diseases, no single biomarker was identified that could specify vulnerable subjects regarding the prenatal distress-offspring's allergic diseases relationship. Some markers are currently known to be elevated in subjects who are prenatally distressed or who are at risk of developing a later allergy. First, genetic polymorphisms in offspring's blood can explain the different effect size in response to a specific exposure.6667 These can synergistically or antagonistically interact with environmental risk factors. Secondly, placental biomarkers deserve attention. Since the mother and fetus are connected through the placenta, the possible pathway through which the maternal distress influences offspring's allergic diseases may involve changes in the placenta. Based on the suggested mechanism, placental HSD2 or oxidative markers in the placenta may reflect in-utero exposures and can quantify the risk for later disease development.5 Furthermore, in some studies, immune markers in cord blood have been regarded as surrogate markers for later allergy development.1920
Other than allergic diseases, epigenetic changes, including methylation status in placenta or cord blood, are now actively being investigated as markers for later disease development.68 In some cohorts, infant stool samples are actively gathered and metagenomically analyzed to explain individual differences in outcomes despite very similar exposures. From offspring's side, markers for stress-reactivity, such as cortisol levels in saliva, are good candidate biomarkers for prenatal distress and later disease development.69 Moreover, as another marker of early exposure and later disease potential, telomere shortening is noticeable for predicting development of noncommunicable disease. 70 The role of these biomarkers, however, has not been verified in the development allergic diseases and now warrants attention.
CONCLUSION
Current evidence had succeeded in demonstrating a close association between prenatal maternal distress and the development of allergic diseases in offspring. However, recall bias must be avoided to ensure a causal relationship by gathering information on maternal distress prenatally. Furthermore, environmental modifying factors, including air pollution, diet, or postnatal distress, should be adjusted for during the analysis. Considering the complex and ambiguous relationship between stress, allergic diseases, and other potentially modifying factors, a population-based prospective birth cohort study could verify a causal relationship between prenatal distress and allergic diseases in offspring; this should also be replicated in another cohort study. In spite of this epidemiologic evidence, researchers have not demonstrated direct evidence that intervention strategies that restore altered stress response systems during the maternal or early infant period can reverse the risk of allergy development. Further studies are needed to clarify the efficacy of intervention strategies.
 XML Download
XML Download