

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Metabolic syndrome (MS) is a group of conditions including abdominal obesity, dyslipidemia, hypertension, insulin resistance, and hyperglycemia, which increase the risk of CVD when they occur together [1-3]. According to a cohort study conducted in the US [4] and Europe [5], men with MS have 2-3 times greater probability for CVD than those without MS. The prevalence of MS among Korean men in 2005 was 32.9% by the Korean National Health and Nutrition Examination Survey, and this increasing prevalence is a growing health issue [6]. Unhealthy lifestyle characteristics such as an unbalanced diet and drinking and smoking habits are the main causes of MS in Korean men [7]. Health care professionals are conducting early identification and treatment of MS to prevent an epidemic increase in CVD.
The Framingham risk score (FRS) is a simplified coronary prediction tool developed to enable clinicians to assess the risk of a cardiovascular event and to identify candidate patients for risk factor modifications worldwide [8-11]. The FRS considers six coronary risk factors, including age, gender, total cholesterol (TC), high density lipoprotein (HDL)-cholesterol, systolic blood pressure, and smoking habits [12], without considering dietary risk factors.
Many studies have shown an association between diet, lifestyle, and the incidence of CVD [13,14]. The National Cholesterol Education Program Adult Treatment Panel III recommended lifestyle modifications, such as diet and weight control, as CVD treatment [15]. Increasing evidence shows that diet modifications have favorable health effects and can prevent the development and progression of CVD. Furthermore, greater adherence to healthy dietary patterns, such as the traditional Mediterranean diet, has been associated with lower mortality rates and a lower incidence of CVD [16-18]. Dietary intake and MS patterns in Korean men have been analyzed in several cohort and case studies [19-21], but no studies have evaluated whether dietary factors are related to FRS or which nutrients are correlated with FRS in Koreans. Considering the prevalent use of FRS to predict CVD and to modify health-risk lifestyle modifications in clinical practice, dietary analyses according to FRS may be necessary to further address the modifiable dietary risk factors and to decrease the epidemic CVD burden.
Substantial evidence suggests that chronic inflammation is an important factor in the initiation and progression of CVD. Acute inflammatory biomarkers, such as high sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6), are sensitive markers that predict the risk for developing CVD [22-24]. Similarly, an elevated level of plasma adiponectin, an antiatherogenic adipokine, is a predictor of decreased coronary heart disease risk [25]. Although inflammatory markers and the FRS predict vascular risk, the association between FRS with hs-CRP is inconsistent, with some reports indicating an association between circulating hs-CRP and FRS [11], whereas other studies have not found a significant association [26]. Some of these discrepancies may be explained by the different study populations. However, there are still an insufficient number of studies on the relationship between inflammatory markers and FRS.
Thus, we investigated the relationship between FRS and dietary factors in Korean men with MS espousing health risk factors for CVD. We also determined whether inflammatory biomarkers were correlated with predicting CHD risk as assessed by the FRS in Korean men with MS.
Subjects and Methods
Subjects
This cross-sectionally designed study was performed with subjects who underwent an annual health examination and voluntarily participated in a dietary modification program conducted at the Bundang Seoul National University Health Promotion Center [27] and Iksan Public Health Center. In total, 180 male subjects (age range, 20-65 yr) were recruited. Men were eligible if they met the MS criteria and exhibited more than three of the five factors reported in the joint interim statement from the International Diabetes Federation and the American Heart Association/National Heart, Lung, and Blood Institute [28]. There criteria were defined as triglyceride concentration ≥ 150 mg/dL, HDL-cholesterol concentration < 40 mg/dL, fasting glucose concentrations ≥ 100 mg/dL or taking antidiabetic drugs, systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 85 mmHg or taking anti-hypertensive drugs, and waist circumference ≥ 90 cm. Exclusion criteria were individuals with CVD, cerebrovascular disease, diabetes complications, or systemic disorders such as severe hepatic, renal, or hematologic diseases. Written informed consent was obtained from all participants, and this study was conducted in accordance with the guidelines of the institutional review board at each clinical center.
Data collection and laboratory analyses
Anthropometic measurements, a food frequency questionnaire (FFQ), and blood samples were collected. A self-administered questionnaire was used to obtain a history of smoking, alcohol drinking, and exercise. Participants were asked to complete the semiquantitative FFQ using the prior 1 year as a reference time point for the nutrient intake analysis [29]. The participants described portion size and consumption frequency of 103 foods items by choosing one of nine options (almost null, 1 time/month, 2-3 times/month, 1-2 times/week, 3-4 times/week, 5-6 times/week, 1 time/day, 2 times/day, or 3 times/day). The FFQ was used to assess average intake, which was converted to nutrient intake using a computerized nutrient analysis program. The Index of Nutritional Quality (INQ) was calculated to assess the adequacy of dietary intake [30]:

Participants were first asked whether they had ever smoked or consumed alcoholic beverages. Past smokers and alcohol drinkers were asked about their age when they quit smoking or drinking. Information on physical activity was elicited, and the frequency and types of exercise were collected. Trained technicians obtained height and weight using an automatic recorder (DS-102, Jenix Co, Seoul, Korea) while participants wore light clothing without shoes. Body mass index (BMI) was calculated as weight divided by height squared. A fiber glass tape measure was used to measure waist circumferences at the point midway between the last rib and the iliac crest. Blood pressure measurements were taken using an automatic blood pressure monitor (Sysmex Co, Kobe, Japan) after > 5 min of rest. All blood samples were obtained from participants in the morning after a 12 hr overnight fast. Blood samples were centrifuged at 3,000 rpm for 15 minutes within 1 hr of collection and stored at -80℃ until analysis. Total and HDL-cholesterol, triglycerides, glucose, uric acid, λ-glutamyl transferase (λ-GT), and glycated hemoglobin were measured with an automated chemistry analyzer (BS-220, Mindray, Shezhen, China). Low density lipoprotein (LDL)-cholesterol concentrations were calculated using the Friedewald equation. Serum hs-CRP was measured by a latex agglutination immunoassay and an automatic analyzer (7600-110, Hitachi, Tokyo, Japan). Serum IL-6 was measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Bender Medisystems, Vienna, Austria). Adiponectin was estimated using an enzyme immunoassay with an ELISA kit (Adipogen Inc, Seoul, Korea).
Assessment of cardiovascular risk
The FRS was calculated by adding the scores based on six coronary risk factors, including age, gender, TC, HDL-cholesterol, systolic blood pressure, and smoking habit. The following cutoffs were used to calculate the FRS: for TC: < 160, 160-199, 200-239, 240-279, and ≥ 280 mg/dL; for systolic blood pressure: < 120, 120-129, 130-139, 140-159, and ≥ 160 mmHg; and for HDL-C: < 40, 40-49, 50-59 and ≥ 60 mg/dL. Ten year risk in percentage was calculated by total points (1 point, 6%; 2 points, 8%; 3 points, 10%; 4 points, 12%; 5 points, 16%; 6 points, 20%; 7 points, 25%; 10 points or more, > 30%). Absolute CVD risk percentage over 10 years was classified as low risk (< 10%), intermediate risk (10-20%), and high risk (> 20%) [12].
Statistical analysis
An analysis of variance was used to test for differences in anthropometric, biochemical, daily dietary intake, and INQ across the three groups, and post-hoc analyses were performed with Tukey's test. Categorical variables were compared with the χ2 test. Analysis of covariance (ANCOVA) was used to examine the relationship between FRS and inflammatory markers, considering the important covariates. Covariates included as potential confounders were age, BMI, and waist circumference. The first model compared only inflammatory markers with BMI across the three groups. The next model included age, and the succeeding model added waist circumference. Significant differences identified by ANCOVA were assessed by Bonferroni post-hoc test. hs-CRP and IL-6 were log transformed before analysis due to skewness in their distributions. A hierarchical multiple linear regression model with FRS as the dependent variable was used to predict whether the FRS was related to inflammatory markers and dietary intake. All independent variables with a correlation coefficient with FRS of up to 0.1 were entered into the model. Dietary intake such as fiber, iron, niacin, vitamin C, folate, vitamin E, and polyunsaturated fatty acids (PUFAs) were entered into model 1, and then log IL-6 and log adiponectin values were factored into model 2. All statistical analyses were performed using SPSS software version 12.0 (SPSS Inc, Chicago, IL, USA). A P < 0.05 was considered significantly different.
Results
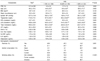
The demographic, anthropometric, and biochemical characteristics of the participants by FRS are shown in Table 1. Fifty-six percent of the subjects (n = 100) were in the low risk (< 10%), 32% (n = 58) were in the intermediate risk (10-20%), and 12% (n = 22) were in the high risk (> 20%) categories. Participants with lower risk had significantly lower systolic blood pressure, and triglyceride, LDL-cholesterol, and total cholesterol levels than those in participants with a higher FRS. No significant differences were observed in serum λ-GT, uric acid, hs-CRP, IL-6, or adiponectin among the groups. The proportion of smoking patients was significantly different between the groups stratified by the FRS levels; however, the proportion of patients that exercised and consumed alcohol was not significantly different between the groups.
Nutrients intake did not differ significantly between the groups (Table 2). According to the dietary quality assessment, all subjects showed a INQ value > 1.0 for protein, phosphorus, iron, zinc, vitamin B1, vitamin B6, niacin, and vitamin C. However, the INQ of calcium, vitamin A, vitamin B2, and folate were < 1.0. Significant differences were observed in the INQ for nutrients between the classified FRS risk groups (P < 0.05). Protein, phosphorus, iron, vitamin A, vitamin B1, niacin, vitamin B6, and vitamin C were consumed at higher levels in the lower risk group than those in the highest risk groups (P < 0.05).
The means of various inflammatory markers across the three groups are shown in Table 3. Model 1 was adjusted for BMI, model 2 was further adjusted for age, and model 3 was further adjusted for waist circumference. No significant differences were seen in mean hs-CRP or adiponectin levels across the three groups, even after adjusting for covariates. However, IL-6 concentrations were significantly lower in subjects with a < 10% FRS than in subjects who were 10-20% FRS or > 20% FRS (0.91 ± 0.26 vs. 1.48 ± 033 vs. 2.72 ± 0.57 pg/mL, respectively; P < 0.05) after adjusting for age, BMI, and waist circumference.
The effects of factors associated with the FRS in patients with MS are shown in Table 4. The relative contribution of each variable related to the FRS was evaluated in a stepwise multiple linear regression analysis. In model 1, which included dietary factors, PUFA explained 3.6% of the variance in FRS. After entering IL-6 (model 2), the total variance explained by the model changed to 6.6%. In this model, log transformed IL-6 was positively related to the FRS (β = 2.135, P = 0.021), whereas dietary PUFA intake was inversely correlated with the FRS (β = -584, P = 0.006).
Discussion
Based on the prevalent worldwide health problem of CVD, researchers have been interested in elucidating CVD risk factors by assessing diet and inflammatory status in patients with MS. We hypothesized that people at high risk for CVD have higher levels of inflammatory markers and pro-inflammatory dietary patterns. As a result, we found that dietary intake in the higher CVD risk groups was poorer than that in the lower risk group, and FRS was independently associated with IL-6 levels after considering age and anthropometric measurements.
Several studies have shown that FRS differs by disease status. According to the Korean National Health and Nutrition Examination Survey, the mean CVD risk by the FRS in Korean men is only 5.11% in office workers and 7.03% in labor workers [31]. Approximately 87% of healthy men were in the low risk group (< 10%) in a study by Kim et al. [32]; however, the mean FRS was 15.3% in patients with diabetes (age, 57.4 ± 16.0 yr) [33]. In our study, the mean FRS was 9.13% and 12% of subjects belonged to the high risk (> 20%) group and 56% of them belonged to the low risk group (< 10%). Therefore, our results show that a higher mean FRS and ratio in the high risk criteria (> 20%) were seen in patients with MS than those in healthy subjects. MS is associated with accelerated atherosclerosis and CVD. Several studies have reported that the main pathogenic mechanism of MS is related to low level inflammation and oxidative stress [34-36]. Excessive abdominal fat accumulation may cause free radical production, innate oxidative damage, and chronic low-level inflammation in patients with MS. hs-CRP is a sensitive acute-phase protein that directly induces atherogenesis by disturbing endothelial function. In epidemiological studies, elevated levels of hs-CRP are associated with an increased risk for CVD [37]. In addition, CRP levels are significantly correlated with FRS in the Caucasian population, and have been used as an adjunctive indicator for global risk prediction of CVD [11]. In this study, we did not reveal a relationship between FRS and hs-CRP. Consistent with our observations, a study conducted by Alissa et al. [26] was unable to show a positive association between FRS and hs-CRP in Saudi men. The FRS is frequently used as a noninvasive screening tool to measure CVD risk in clinical practice and public health research; however, the predictive ability of the FRS varies between populations, ethnic groups, and socio-economic status [38,39]. This could be an explanation for this discrepancy between hs-CRP levels and the FRS in our study.
IL-6 levels are a CVD risk factor [24], and IL-6 has prominent effects on arterial intima-media thickness and pulse wave velocity in Japanese men [40]. In a meta-analysis, IL-6 levels showed a strong association with an increased incidence of CVD [41]. We found that IL-6 levels were associated with the FRS after adjusting for obesity factors. Because visceral adipose tissue, which secretes several adipokines, may affect CVD risk, we adjusted for BMI and waist circumference to eliminate the effects of adiposity on the FRS. Our results suggest that serum IL-6 concentration might be more sensitive than that of hs-CRP for detecting CVD risk and recommend an evaluation of IL-6 as a potential adjunct for predicting CVD with the FRS in men with MS.
Adiponectin functions as an anti CVD protein by increasing fatty acid oxidation and improving insulin sensitivity [25,42]; however, we were unable to show an inverse association between FRS and adiponectin in men with MS. This may have been because our subjects were selected men with MS, who were insulin resistant, which may have attenuated the relationship between adiponectin and FRS.
INQ is used to calculate dietary quality by eliminating the calorie effect. We found that most INQ values of nutrients were > 1.0, except calcium, folate, vitamin A, and vitamin B2. We also showed that dietary quality, assessed by INQ, was lower in the higher CVD risk groups than that in the lower risk groups. There is an inverse association between calcium intake and CVD mortality [43], and calcium supplementation may prevent absorption of saturated fatty acids resulting in a reduction in TC and LDL-cholesterol levels [44]. A folate deficiency can be a risk factor for CVD by preventing metabolism of homocysteine to methionine, and further inducing oxidative stress and altered lipid metabolism [45]. Therefore, nutritional education should be actively attempted to provide a healthy dietary intake with focus on insufficient nutrients to CVD-susceptible men with MS before the onset of clinical symptoms.
Dietary patterns low in natural antioxidants, such as the lack of consumption of fruits and vegetables, in patients with MS may activate the innate inflammatory response, most likely due to excess production of proinflammatory cytokines, which induce vascular endothelial dysfunction and ultimately increase the incidence of CVD [46]. In a study by Palmieri et al., serum concentrations of vitamin C and α-tocopherol in patients with MS were lower than those in control subjects [36]. In this study, we found that the INQ of vitamin C was inversely associated with FRS. Vitamin C is a water-soluble antioxidant with possible preventive effects as it restores vitamin E to its antioxidizing state, thereby lowering the oxidized LDL cholesterol and malondialdehyde levels and elevating the levels of glutathione peroxidase and superoxide dismutase [47]. Vitamin C also appears to be important for preventing CVD, as it improves arterial elasticity through arterial vasodilatation [48]. Furthermore, cigarette smokers and alcoholics are at risk for low vitamin C status [49,50]. In our study, vitamin C was appropriately consumed at a mean concentration of 101 mg/day, as compared to the mean daily-recommended nutrient intake of 100 mg proposed by the Korean Dietary Reference Intakes [51]. However, considering that vitamin intake was less than the recommended nutrient intake (82.4 mg/day) and that 86.7% and 73.3% of subjects were current smokers and alcohol drinkers in the highest FRS group, respectively, there is a need to ascertain the provision of sufficient levels of vitamin C to minimize oxidative stress in patients at high-risk for CVD.
Considerable evidence shows that a diet enriched with n-3 fatty acids protects against atherosclerosis and that PUFAs are effective in lowering LDL-cholesterol [52]. Dietary fatty acids modulate lipoprotein concentrations as well as inflammatory and endothelial function [53]. Our findings confirmed previous observations by providing a negative correlation between PUFA intake and the FRS in patients with MS.
We acknowledge the following limitations in this study. This was a cross-sectional rather than a prospective study; thus, we were unable to identify a causal relationship between inflammatory markers and FRS. Another limitation is that the subjects consisted of patients who visited a health promotion center, so selection was biased. However, the present study has a strength in that it is the first study to examine the FRS and dietary intakes for a better understanding of the associations between dietary differences and CVD risk.
In conclusion, our results suggest that categorizing CVD risk by the FRS is related to serum IL-6 concentrations and can be used to estimate dietary insufficiencies in Korean men with MS and a higher risk for CVD.



 XML Download
XML Download