

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sertoli cell tumors are very rare and account for only 1 percent of all testicular neoplasms. Ten percent of these tumors metastasize and are considered malignant. They can be found at any age, but most occur in the age range of 30 to 40 years. The most common clinical finding is a painless scrotal mass, and one-third are associated with gynecomastia and hormonal imbalance. Treatment of benign Sertoli cell tumors is radical orchiectomy. If pelvic lymphatic metastasis is present, pelvic lymph node dissection is usually done, but the effect of radiation and chemotherapy is questionable.1 A review of the Korean literature showed 2 cases of malignant Sertoli cell tumors and 1 case of a benign tumor in Korea.2-4 Here we report the case of a 46-year-old man with a Sertoli cell tumor of the testis and review the literature.
CASE REPORT
A 46-year-old man visited the urology clinic with a complaint of a left scrotal mass. He had discovered a hard mass in his left scrotum 4 years previously but he had not visited the urology clinic because the mass was asymptomatic. Physical examination revealed a 1.5 cm, well-defined, hard, painless mass. There was no sign of gynecomastia or other feminization. There was no scrotal trauma or other medical problems on his past history.
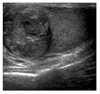
Serum α-fetoprotein, β-human chorionic gonadotropin, and lactate dehydrogenase were 4.26 IU/ml, 1 mIU/ml, and 397 IU/l, respectively, which were within the normal limits. Serum luteinizing hormone (LH) was slightly elevated (6.22 mIU/ml), but serum follicle stimulating hormone (FSH), prolactin, testosterone, and estradiol were normal. Ultrasonography revealed a 1.5×1.5 cm, well-defined mass with irregular echogenicity in the left testis (Fig. 1).
We planned to perform either a radical orchiectomy or organ-sparing surgery on the basis of the frozen biopsy results. On gross examination, the mass was 1.7×1.3 cm in size with a white-yellow color and a hard nodular appearance. There was no gross hemorrhage or necrosis in the mass of testis. The specimen was examined quickly by using frozen section analysis. It was proven to be a Sertoli cell tumor, and the patient underwent a radical orchiectomy. Microscopically, the mass was confined in the testicle and there was no invasion to the tunica albuginea or epididymis. The testicular tumor showed a cord of cells with abundant eosinophilic cytoplasm, had prominent centrally located nucleoli, and was surrounded by stromal cells. There was no evidence of malignancy, such as morphological abnormality, necrosis, mitosis, vascular invasion, or solid structure (Fig. 2). Immunohistochemical staining was positive for vimentin and cytokeratin and focally positive for S-100 but negative for C-kit and SMA (Fig. 3).
Chest X-ray and abdominopelvic CT scan revealed no evidence of lymphatic or distant metastasis. The patient continues with his follow-up 6 months postoperatively, and no recurrence has been observed.
DISCUSSION
Sertoli cell tumors are very rare and account for only 1 percent of all testicular neoplasms. These tumors can occur at any age, including in newborns, but the peak incidence of Sertoli cell tumors is in the 30s and 40s. The etiology of testicular cancer is unknown. Although most Sertoli cell tumors develop in normal testis, there are some reports of these tumors in undescended testis.5
The most common clinical feature of Sertoli tumors is a "slow growing painless testicular mass." About one-third of Sertoli cell tumors are associated with gynecomastia derived by estrogen production, but it is not clear that estrogen is produced by Sertoli cells or stromal cells.1 Forty percent of benign Sertoli cell tumors are associated with genetic syndromes such as Carney syndrome and Peutz-Jeghers syndrome; these phenomenon are more common in bilateral or multiple tumors.6 In the present case, the patient was 46 years old and presented with a painless testicular mass without hormonal abnormalities or gynecomastia.
Most Sertoli cell tumors fall into the "not otherwise specified", or NOS, category, but subsets are represented by 2 variants: the sclerosing Sertoli cell tumor (SSCT) and the large cell calcifying Sertoli cell tumor (LCCSCT). These 2 variants are determined by histologic features of Sertoli cell-like epithelial components and stromal components. LCCSCTs are characterized histologically by large tumor cells, abundant eosinophilic cytoplasm, tubular and trabecular differentiation, and extensive calcified debris. SSCTs are characterized histologically by solid and hollow, simple and anastomosing tubules; large irregular aggregates; and thin cords of Sertoli cells in a prominent collagenous background.7 Immunohistochemical staining may add some differential diagnostic information from other testicular tumors. Sertoli cell tumors are usually positive for cytokeratin and vimentin and weakly positive for S-100.5 Our patient was diagnosed as having a Sertoli cell tumor NOS because the tumor was positive for cytokeratin and vimentin and weakly positive for S-100 and there was no calcified lesion or prominent collagenous background.
A large tumor size, irregular margin of tumor, invasion to adjacent tissue, lymphatic or vascular invasion, and mitotic figure usually indicate a malignant Sertoli cell tumor, but metastasis is essential to prove a clinically malignant tumor.1,5 Most Sertoli cell tumors are benign, but 10 percent of Sertoli cell tumors present with distant metastasis, and late metastasis has been reported during follow-up after radical orchiectomy. Young et al,5 in their mean 3.8 year follow-up of 16 patients with Sertoli cell tumors after radical orchiectomy, reported that 3 of 12 patients who had no metastasis at presentation were found to have late metastasis. The histologic findings of these 3 patients showed microvascular invasion in 2, nuclear pleomorphism in 2, and necrosis in 1 patient. Eight of 9 patients who had a benign clinical course presented with a tumor less than 5 cm, but 4 of 7 patients who had metastasis presented with a tumor of more than 5 cm; data on tumor size were not available for 3 patients. Metastasis was found in the retroperitoneal lymph nodes in 6 patients, in the lung in 4, in the inguinal lymph node in 3, in the rib and supraclavicular lymph node in 2, and in the vertebra and liver in 1 patient.
The prognosis of a benign Sertoli cell tumor is good, but the prognosis of malignant Sertoli cell tumors has not been established. Metastatic Sertoli cell tumors have a poor prognosis; Godec8 reported a mean 15 month survival period after diagnosis of metastasis in 9 patients.
Although metastasis is the only evidence of malignancy in Sertoli cell tumors, there are some reports of late metastasis. The latest metastasis reported in the literature occurred 10 years after radical orchiectomy.9 Kolon et al10 suggested that a minimal 5 years of follow-up is necessary because of tumor characteristics.
In our case, we think that the prognosis of our patient will be good because of the small size of the mass, the lack of any histologic abnormalities indicating malignancy, and no evidence of metastasis. But close follow-up will be necessary for detecting late metastasis.


 XML Download
XML Download