

 PDF
PDF Citation
Citation Print
Print



Introduction
Most patients experience anxiety and stress before anesthesia and surgery [1]. Traditionally, benzodiazepine premedication has been used to prevent adverse effects from preoperative anxiety [23]. Recently, however, the use of benzodiazepines has declined in healthy adult patients. This could be due to concerns about potential oversedation before anesthesia, delayed recovery from anesthesia, and impairment of psychomotor function in the early postoperative period [4]. Nevertheless, anxiolysis with an adequate dose of benzodiazepine may lead to a more hemodynamically stable induction of anesthesia [56] and improved general wellbeing of patients, and patient satisfaction [7].
Midazolam is the most commonly administered benzodiazepine, especially via the oral route [8]; however, benzodiazepine as an oral tablet is not currently available in South Korea. Similar to midazolam, triazolam is a short-acting benzodiazepine that has been used in various clinical fields [910]. However, only a limited number of studies have examined the use of oral triazolam premedication before general anesthesia [1112]. In our previous study compared the use of triazolam 0.25 mg and alprazolam 0.5 mg as oral premedications, no significant differences in anxiety or sedation were observed between the two groups, or in within-group analyses (before versus after premedication) [13]. We assumed that these neutral results might have been due to the lack of a comparable control group or insufficient drug dose, because triazolam is known to possess anxiolytic, sedative and amnesic properties that also characterize other benzodiazepines [1014].
Therefore, the present study included a no premedication group, as well as usual- and high-dose triazolam premedication groups. The primary endpoint was to clarify the effectiveness of triazolam premedication for adults, with respect to factors such as anxiety, sedation, and amnesia. We also evaluated the effects of triazolam on anesthetic recovery, psychomotor performance and patient satisfaction.
Materials and Methods
Ninety patients, of American Society of Anesthesiologists physical status classification I–II, who were aged 20–55 and were scheduled for elective surgery under general anesthesia, were enrolled. Patients who took analgesic, sedative, antidepressant, or antiepileptic drugs within the week before surgery were excluded. The study was approved by the Institutional Review Board of our institution and National Research Institute of Health (KCT0001720, https://cris.nih.go.kr/cris/en/).
On the evening prior to surgery, a routine preoperative visit was performed by the assigned anesthesiologist, with written informed consent for study participation and anesthesia obtained separately. A research nurse then evaluated the patient's baseline level of anxiety, sedation, psychomotor performance, and hemodynamic variables such as systolic blood pressure and heart rate. The level of anxiety was determined using a 7-point scale (0, calm and relaxed; 1, apprehension; 2, mild anxiety with unsteady eyes; 3, moderate anxiety with body shaking; 4, verbally expressing anxiety without being asked; 5, severe anxiety; and 6, crying) [1315]. The level of sedation was determined by a 5-point scale (0, alert; 1, aroused by voices; 2, aroused by gentle tactile stimulation; 3, aroused by vigorous stimulation; and 4, lack of responsiveness) [13]. Because psychomotor performance (visual-motor coordination) may be affected by the perioperative use of benzodiazepines, we evaluated it using a Digit Symbol Substitution Test (DSST) [1316]. The DSST consists of digit-symbol pairs (e.g., 1/-, 2/┴ . . . 7/Λ, 8/X, 9/=) followed by a list of 20 digits. The patient was asked to write the corresponding symbol under each digit as fast as possible, and the completion time was recorded.
On the day of surgery, patients were allocated to receive no premedication (control group), or oral triazolam (Halcion®; Pfizer, New York, NY, USA) 0.25 mg (T0.25 group) or 0.375 mg (T0.375 group) according to a computer-generated randomization list. The study drug was administered 1 h before transfer to the operating room, because a plateau concentration of oral triazolam is achieved in 30 min and maintained for 180 min [17]. Upon patient arrival in the operating room, the same research nurse evaluated the patient's level of anxiety, sedation, psychomotor performance, and hemodynamic variables. In a memory test used to detect amnesia, the research nurse showed each patient an object, such as a stethoscope, while saying the name of object, and asked the patient to remember it [13]. Then, a bispectral index sensor (BIS®, Aspect Medical Systems, Norwood, MA, USA) was applied and patients were asked to keep their eyes closed. To confirm the accuracy of the measurement, a BIS value was obtained when the signal quality exceeded 50. General anesthesia was induced with 2.0 mg/kg intravenous propofol, and endotracheal intubation was facilitated by rocuronium 0.8 mg/kg. Anesthesia was maintained with desflurane (4–5 vol%) and remifentanil to achieve BIS values between 40 and 60. At the end of surgery, serotonin type 3 antagonists were given to the patient to prevent postoperative nausea and vomiting. Residual neuromuscular block was reversed with pyridostigmine and glycopyrrolate. After tracheal extubation, the patient was transported to the postanesthesia care unit (PACU), where consciousness scores were recorded every 15 min (0, unresponsive; 1, aroused by calling; 2, fully awake). The incidence of nausea and vomiting was recorded during the PACU stay. When the patient was ready for discharge, the PACU stay time was recorded and psychomotor performance was re-evaluated.
On the next day of surgery, the research nurse asked each patient whether he/she remembered being moved from the ward to the operating room and inquired about the object shown before anesthesia. When the patient could not remember either of these, amnesia was confirmed. The psychomotor performance and patient satisfaction score concerning overall anesthesia care (0, unsatisfactory; 1, fair; 2, good, 3; excellent) were also evaluated.
The sample size was calculated using data from a preliminary study, which suggested a 0.4-fold difference in the proportion of patients with increased anxiety in the operating room between the no premedication and triazolam 0.25 mg groups. For a two-sided test of difference, using α = 0.016 (error type I/number of comparisons = 0.05/3) and β = 0.2 for each comparison, the required sample size was estimated to be 28 evaluable patients per group. Assuming a dropout rate of 5%, we planned to recruit 30 patients to each group. Differences among the groups were assessed by one-way analysis of variance (ANOVA) or Student's t-test for normally distributed variables, by the Kruskal-Wallis test for non-normally distributed variables, and by Fisher's exact test or the linear-by-linear association test for categorical variables. The DSST completion times, as an index of psychomotor performance, were compared using repeated measures ANOVA. Spearman's correlation coefficients were calculated for all measured variables. SPSS for Windows software (ver. 20.0, IBM Corp., Armonk, NY, USA) was used for statistical analyses. P values less than 0.05 were considered statistically significant.
Results
The three groups were similar with respect to age, gender, weight, operation site, and duration of anesthesia (Table 1). Time intervals from medication to arrival in the operating room were also similar between both triazolam groups. In total, 15.6% of patients (14 out of 90) were excluded due to patient refusal (n = 3), follow-up failure (n = 4), randomization error (n = 3), and an inadequate time interval from medication to arrival in the operating room (n = 4).
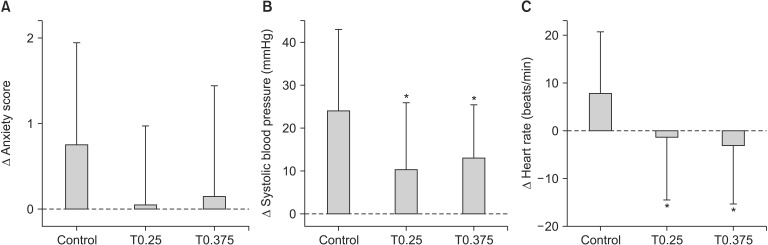
Baseline anxiety score, systolic blood pressure and heart rate measured on the evening prior to surgery were similar among the groups (Table 2). Upon arrival in the operating room, the proportion of patients showing increased anxiety in the control, T0.25 and T0.375 groups was 58.3% (n = 14), 32.0% (n = 8), and 40.1% (n = 11), respectively; these differences were not statistically significant (P = 0.167). The changes in anxiety scores from baseline were also not statistically different among the groups (P = 0.055). However, systolic blood pressure and heart rate showed marked increases in the control group, whereas the corresponding increases were significantly lower in the T0.25 and T0.375 groups (Fig. 1).
Most patients were alert (sedation score = 0), although seven patients in the triazolam groups were minimally sedated and aroused by voices (sedation score = 1). The presence of sedation (sedation score ≥ 1) and BIS values before anesthesia induction were not significantly different among the groups (Table 2). However, there was a positive correlation between triazolam dose and the number of patients with BIS values < 90 (linear-by-linear association, P = 0.039). The incidence of amnesia was also dose-dependent (linear-by-linear association, P = 0.001), and significantly higher in the T0.25 and T0.375 groups (Table 2). No patient showed amnesia in the control group. Except for the dose-dependent increase in the number of patients with amnesia and BIS values < 90, there were no significant differences in outcomes between the T0.25 and T0.375 groups.
Delayed recovery from general anesthesia was not observed in any study group with respect to the time from end of surgery to PACU admission, PACU stay time, and consciousness scores in the PACU (Table 3). The rate of return to baseline psychomotor performance, as assessed by the DSST completion time was also similar among the groups. The incidence of nausea was 16.7% in the control group compared with 0% in the T0.25 group and 3.7% in the T0.375 group (P = 0.039); however, post hoc analysis with Bonferroni correction did not reach statistical significance. In all patients, no respiratory depression was observed in the preoperative or postoperative period.
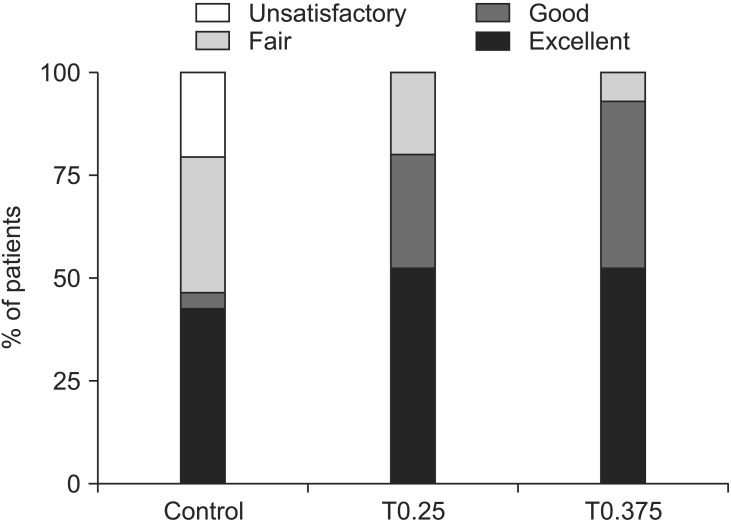
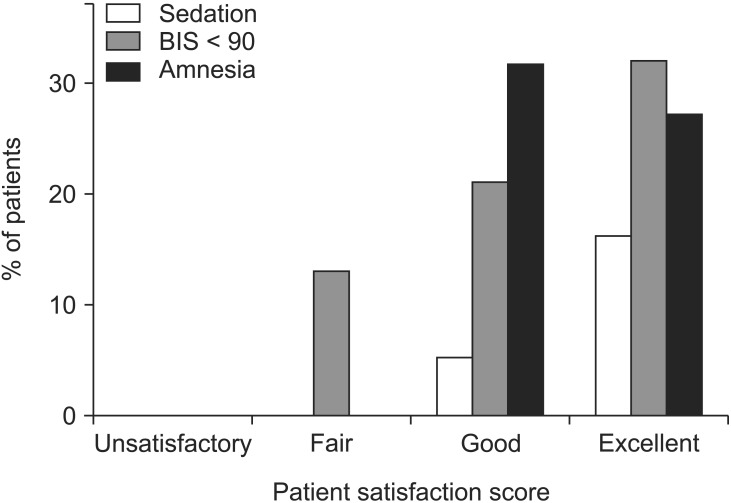
Regarding patient satisfaction scores for overall anesthesia care, the mean scores were not significantly different among the groups, although the T0.25 and T0.375 groups showed a significantly higher incidence of high scores (≥ 2) compared with the control group (Table 4, Fig. 2). Satisfaction scores were also correlated with the presence of sedation (≥ 1), as well as with the number of patients with a BIS value < 90 and amnesia (P < 0.05, Spearman correlation coefficient = 0.243, 0.227 and 0.228, respectively) (Fig. 3).
Discussion
This clinical study evaluated the effect of oral triazolam premedication at 0.25 mg and 0.375 mg on anxiety, sedation, and amnesia in adults undergoing general anesthesia. Previous studies have demonstrated that triazolam at 0.25 mg has significant anxiolytic and sedative effects [1118]. In contrast, Baughman et al. [12] reported that those effects were significant only at 0.5 mg. However, Longbottom and Pleuvry [19] showed that triazolam at 0.5 mg produced significantly prolonged cognitive deficits, despite a better sedative effect compared with 0.25 mg. Therefore, we selected the usual recommended dose of 0.25 mg, as well as a slightly higher dose of 0.375 mg, rather than the maximum permissible dose of 0.5 mg to reduce unnecessary complications.
In the present study, both triazolam 0.25 mg and 0.375 mg significantly lessened the increase of systolic blood pressure and heart rate before anesthesia induction. Since such hemodynamic changes have been used as physiologic indicators of anxiety response [2021], this finding suggests that triazolam has a clinically meaningful anxiolytic effect. In terms of the anxiety score, the level of anxiety in both triazolam groups was generally lower than that in the control group, although the differences were not statistically significant.
Numerous studies have demonstrated a significant sedative effect of triazolam [1118]. In the present study, however, the sedative effects of triazolam at 0.25 mg and 0.375 mg were not prominent in either the subjective (sedation scale) or objective (BIS) assessments. These results correlated with those of our previous study [13], which showed that sedation level did not increase significantly from baseline in the triazolam 0.25 mg group. Baughman et al. [12] also reported that only triazolam at 0.5 mg, and not at 0.25 mg or 0.125 mg, produced more sedation than placebo. Taken together, although a dose-dependent increase in the number of patients with BIS values < 90 was observed in the present study, it is likely that triazolam at below 0.5 mg has a weak sedative effect in adult patients.
Meanwhile, the amnesic effect of triazolam 0.25 mg and 0.375 mg was strong and significant, consistent with previous studies [1113]; it was also dose-dependent. This high amnesic potential could be helpful for patients who have unpleasant memories of the operating room before anesthetic induction [2223]. The correlation analysis in the present study showed that patients who had amnesia, or even weak sedation, tended to report higher levels of satisfaction with overall anesthesia care.
No significant delay in postoperative mental or psychomotor recovery was observed among the healthy young adults included in the present study. However, in elderly populations, and in patients with hepatic dysfunction, greater and prolonged sedation or impairment of psychomotor function could occur due to high plasma concentrations and high sensitivity to triazolam [2425]. Therefore, triazolam should be used cautiously, and with dose adjustment, in such populations.
One interesting finding was that postoperative nausea was less common in the triazolam groups compared with the control group, although the difference did not reach statistical significance. Numerous studies, and a recent meta-analysis including 12 randomized controlled trials, have highlighted the antiemetic properties of benzodiazepines, particularly midazolam, when used in the perioperative period [2627]. Further studies with larger sample sizes and longer follow-ups will be necessary to confirm this potential advantage of triazolam premedication.
The present study had some limitations. First, we compared 0.25 mg and 0.375 mg of triazolam in relatively healthy young adults. To ensure safe and effective use, the effect of various doses in a wide range of populations should be evaluated in future studies. Second, overall anxiety scores in the operating room were low, even in the control group (1.5 ± 1.0 on a 7-point scale). This finding may be explained by the anesthesiologist's preoperative visit as a routine practice in our hospital, which has been shown to reduce preoperative anxiety as effectively as pharmacologic intervention [2829]. Therefore, the anxiolytic effect of triazolam may have been masked by the anxiolytic effect of a preoperative visit; this should be considered by future studies.
In conclusion, triazolam 0.25 mg or 0.375 mg significantly reduced the hemodynamic changes associated with anxiety, produced potent amnesia, and improved patient satisfaction with respect to overall anesthesia care. These favorable effects were not accompanied by oversedation or delayed recovery from general anesthesia. Therefore, we suggest that triazolam can be effective as an anesthetic premedication in adults, especially in countries where oral midazolam is not available.
 XML Download
XML Download