

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Situs inversus is a congenital condition in which the major visceral organs (within the thorax and abdomen) are either reversed or mirrored from their normal positions. When the heart remains on the normal left side of the thorax in the presence of abdominal situs inversus, the condition is known as situs inversus with isolated levocardia.1)2) Severe forms of congenital heart defects are almost always associated with this condition.
Splenic defects such as asplenia and polysplenia are examples of this anomaly. Polysplenia is characterized by a tendency for bilateral left-sidedness, including bilateral two-lobed lungs, interruption of the inferior vena cava (IVC) with azygos continuation, and complex cardiac anomalies.3)4) A combination of abdominal situs inversus with structurally normal levocardia, bilateral bi-lobed lungs, polysplenia, left-sided IVC draining to the right atrium is extremely rare. In this report, we present a case of situs inversus with levocardia, left-sided IVC connecting to the right atrium, and polysplenia, in a 19-year-old male patient. There are few published reports regarding the polysplenia with uninterrupted left-sided IVC and isolated levocardia.5)
Case
A 19-year-old male was referred to the Pediatric Cardiology Clinic of Chonbuk National University Hospital for the evaluation of abnormal chest X-ray films showing the position of the stomach gas as being discordant with the location of the heart. The patient had no cardiac symptoms and was a normal developed adolescent. Family and past histories were negative. Physical examination revealed this young man to be acyanotic and was in no distress. Cardiac examinations revealed a grade 1/6 ejection systolic murmur at the upper left sternal border. The liver dullness was presented in the upper left quadrant of the abdomen. The remaining part of the physical examination was entirely normal.
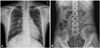
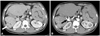
Plain X-ray films of the chest and abdomen showed a normally located heart and a right-sided stomach (Fig. 1). The electrocardiogram was normal with sinus rhythm. Trans-thoracic echocardiographic study demonstrated no intra-cardiac lesions. The IVC was seen on the left side, crossed the midline at the level of the hepatic dome, and connected directly to the right atrium. Spiral computed tomography of the thorax and abdomen showed situs inversus with levocardia and multiple spleens in the right upper quadrant of the abdomen (Fig. 2A), a midline liver, a midline positioned gall bladder, hepatic veins with unusual drainage into the IVC (Fig. 3), and a prominent pancreatic head with associated absence of body and tail of the pancreas. The stomach was located on the right side. Most of small bowel loop was located in the right-lateral portion of the abdomen along the left side ascending colon, with some intestinal malrotation. The splenic artery originated from the celiac trunk of the left sided descending aorta with tortuosity coursing to the spleens. There was a discrete aneurysmal dilatation (2.0×2.6 cm in diameter) in the proximal portion of the artery (Fig. 2B). The IVC ran on the left side (Fig. 4A), and connected directly to the right atrium (Fig. 4B). Azygos and hemiazygos veins, and lumbar veins on both sides were slightly dilated. The ascending aorta, main pulmonary artery, pulmonary veins, and superior vena cava were all normally positioned. The structure of right lung was a mirror to the normal left lung, i.e., bilateral bi-lobed lungs (Fig. 5).
Discussion
Situs inversus with isolated levocardia is an extremely rare anomaly.1) With the heart in a normal position, situs inversus of abdominal organs implies that either situs inversus or situs ambiguus is present. Most cases of situs inversus with levocardia are associated with severe congenital heart defects, either asplenia or polysplenia syndromes with situs inversus or situs ambiguus.2)6)7) Polysplenia is more prevalent in females and shows variable clinical manifestations and prognosis.8) Compared to those in asplenic patients, cardiac anomalies in polysplenic patients are less common and are less complicated.8) In an autopsy of 146 patients with polysplenia, 56% of the subjects had abdominal heterotaxia, 55% had bilateral bi-lobed lungs, and at least half of the patients had cardiac anomalies.9)
Patients with typical polysplenia syndrome tend to exhibit bilateral left-sidedness, with two or more splenic masses and multiple organ anomalies, including severe cyanotic congenital heart defects. 3)4)10) Cardiovascular abnormalities frequently found in polysplenia syndromes include complete endocardial cushion defect, double outlet right ventricle, two left atria (with absent sinus node and thus with junctional rhythm), single or common atria, pulmonary stenosis or atresia, pulmonary venous anomalies, and interrupted IVC with azygos continuation. The interrupted IVC is one of the most frequent abnormalities that help distinguish polysplenia from asplenia syndrome. Bilateral bi-lobed lungs (two left lungs) with hyparterial bronchi are usually present. The liver is often symmetric. The abdominal viscera may be only partially inverted or completely inverted. The intestines often show varying degrees of malrotation,1) which is seen in approximately 70% of patients with asplenia and polysplenia syndromes.11)
One of the most consistent abnormalities seen in polysplenia syndrome is the interrupted IVC. Even when the structure of the lungs and heart are normal, the IVC usually does not connect directly to the right atrium. Instead, it continues as the azygos or hemiazygos veins and connects to the superior vena cava (azygos or hemiazygos connection). The hepatic vein does not connect to the IVC; instead, it drains directly to the right atrium. Direct connection of the left-sided IVC to the right atrium, as seen in our case, is extremely rare.5)
The exact cause of situs inversus with levocardia is not fully understood.7) For asymmetric organs like the heart, lungs, and digestive system, left-to-right (L-R) patterning is one of the most important events in embryonic development. Proper morphogenesis and positioning of internal organs require delivery and interpretation of precise signals along the left-right axis. The heart begins from primary heart tube that later forms either l-loop or d-loop, and differentiates further through septation of the cardiac chambers and great vessels. An embryonic l-loop is expected to form a mirror image of the normal heart and pivots into the right chest. On the other hand, d-loop is expected to result in normal situs solitus heart in the left chest. The orientation of the abdominal organs may have a separate L-R signaling system which would coordinate normally with the L-R signaling system for the heart. It is not known how the L-R signaling system for the abdominal organs and that for the heart communicate each other and coordinate the information. Failing normal coordination from the two systems may have caused this set of abnormalities through an unknown mechanism.
Prognosis of situs inversus with levocardia largely depends on the severity of associated cardiac anomalies,12) although later developments of bowel obstruction from midgut volvulus13) caused by associated intestinal malrotation may also be life-threatening.12)14) Most patients with the heterotaxy syndromes die in childhood from their complex congenital heart defects. Approximately 10% of patients with polysplenia may reach adulthood without any complications as seen with our case.15) In patients with polysplenia syndrome, abdominal discomfort or pain should be carefully investigated for possible intestinal obstructions or other complications, such as those arising from associated aneurysmal dilatation of the splenic artery.
It is important for practitioners to be aware of the fact that discordant cardiac shadows and stomach bubbles are usually found in association with severe abnormalities of the heart and blood vessels and that the practitioners should carry out a thorough investigation for potential abnormalities.



 XML Download
XML Download