

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ortner syndrome or cardiovocal syndrome is a rare condition characterized by hoarseness of voice associated with cardiovascular pathology. Left recurrent laryngeal nerve palsy is the source of the hoarseness. Mitral stenosis is a common cause, but a myriad of other cardiac and non-cardiac conditions may be responsible as well.
Case
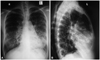
A 35-year-old non-smoker, normotensive female patient presented with progressive breathlessness, recurrent episodes of productive cough and occasional haemoptysis for six months and hoarseness of voice for 1 month. She was on anti-TB drugs with standard regimen for the presumptive diagnosis of pulmonary tuberculosis, to which the response was poor. On examination, she was dyspnoic, mildly anaemic, had early clubbing but was not cyanosed. Her respiratory rate was 22/min, pulse 100/min, regular, blood pressure 100/60 mm of Hg, JVP raised with prominent a wave. There was a tapping apex beat, left parasternal heave, palpable P2 and a diastolic thrill over the apical area. The 1st and the pulmonary component of the 2nd heart sounds were loud, and a low-pitched, localised, mid diastolic murmur of grade 4/6 was heard over the apical area. Her breath sound was vesicular with bilateral coarse crepitations throughout the lower and mid chest. Total leukocyte count was 8000/mm3, erythrocyte sedimentation rate 15 mm in 1st hour, hemoglobin 10.8 gm/dL, C-reactive protein negative, anti-streptolysin O titer <200 IU, bleeding time 4 minutes, clotting time 5 minutes, prothrombin time was normal. Acid-fast bacilli were not found in the sputum and antibodies from lymphocyte secretions for the diagnosis of TB were negative. Ultrasonogram of the whole abdomen was unremarkable. Chest X-ray showed straightening of the left cardiac border and bilateral ring shadows in mid and lower lurg zones (Fig. 1). Echocardiography revealed moderate mitral stenosis with mitral valve area 1.35 cm2, mildly dilated left atrium (41 mm), dilated pulmonary artery and its branches and severe pulmonary hypertension (pulmonary artery systolic pressure, PASP 92 mm Hg). High resolution computed tomography (CT) scan of the chest (Fig. 2) revealed features of bilateral bronchiectasis, whereas CT pulmonary arteriography (Fig. 3) found dilated pulmonary arteries (pulmonary trunk 34 mm, right pulmonary artery 23.8 mm and the left pulmonary artery 18.7 mm). Left vocal cord palsy was detected in fibreoptic laryngoscopy (Fig. 4).
A diagnosis of chronic rheumatic heart disease, moderate mitral stenosis, bilateral bronchiectasis and Ortner syndrome was made. The patient was treated conservatively with rheumatic fever prophylaxis, additional antibiotics on the basis of culture and sensitivity report of sputum, chest physiotherapy, bronchodilators, diuretics and nifedipine. Over the next few months, she improved clinically, PASP came down to 62 mm Hg, but the findings remained unchanged in follow-up chest X-rays, and the hoarseness of voice did not improve significantly. While staying in the village, suddenly her condition deteriorated and on the way to the hospital she expired.
Discussion
Ortner syndrome was first described by Nobert Ortner, a Viennese physician in 1897, in a case of mitral stenosis with dilated left atrium.1) Subsequently, it was reported with mitral stenosis,2)3) mitral regurgitation,4) atrial myxoma,5) primary pulmonary hypertension,6)7) thoracic aortic aneurysm,8)9) aortic dissection,10) pulmonary embolism,11) defibrillation,12) transcatheter ablation of atrial fibrillation,13) cardiothoracic surgery14) and heart-lung transplantation.15) The basic abnormality is paralysis of the left recurrent laryngeal nerve. Though an initially enlarged left atrium was thought to be the main culprit, the current understanding favours pressure in the pulmonary artery playing the most important role in causing the nerve compression in a majority of the cases.10) The incidence of cardiovocal syndrome in mitral stenosis ranges from 0.6% to 5%.16)
The most common manifestation of Ortner syndrome is hoarseness of voice. Unilateral vocal cord paralysis increases the risk of aspiration which may be present in up to 40% of patients.17)
In the present case, the left recurrent laryngeal nerve was most probably compressed by the dilated pulmonary artery, not by the left atrium because the latter was only mildly dilated. Also the moderate mitral stenosis in isolation was unlikely to cause severe pulmonary hypertension. Bilateral bronchiectasis probably contributed to the major share of the severity of pulmonary hypertension which ultimately caused dilatation of the pulmonary arteries. Presence of dual pathology aggravated the situation.
Ortner syndrome is suspected from history and clinical examination; a chest X-ray or CT scans of the chest, fibreoptic laryngoscopy and laryngeal electromyography help confirmation of the diagnosis.18)
The prognosis of recurrent laryngeal nerve paralysis depends on the degree and duration of nerve compression.19) The treatment of unilateral vocal cord palsy consists of early rehabilitation, treatment of the primary etiology and endoscopic insertion of a prosthesis or injection of fat or collagen.10) There are two absolute indications for surgery: aspiration pneumonia and the patient's desire to improve the voice-related quality of life.20) Considering the general condition of the patient, conservative strategy was adopted. Relieve of mitral stenosis by percutaneous transluminal mitral commissurotomy could be done, but in presence of moderate degree of stenosis and high risk from comorbid lung disease, the idea was abandoned. In conclusion, Ortner syndrome is a rare entity. A number of cardiovascular conditions may contribute to its aetiopathogenesis. Presence of dual pathology may make the diagnosis and management difficult and worsen the prognosis.



 XML Download
XML Download