

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Premenstrual syndrome (PMS) is a menstrual disorder that occurs 2–10 days before menstruation. PMS involves a combination of physical, mental, and behavioral symptoms that resolve once menstruation begins [1]. Approximately 80% to 90% of women who have menstruation experience varying degrees of PMS [2] and approximately 5% to 8% of women suffer from severe pain or functional impairment [3]. Of women who experience PMS, students, who undergo physical changes and rapid growth, are particularly hindered in their school lives and daily living because of PMS [4]. Therefore, it is necessary to identify the factors that influence PMS in students attending middle school, as this is generally the period that marks the beginning of puberty.
PMS is influenced by physiological factors, such as body mass index (BMI), age at menarche, family history, sleep pattern, dietary habits, and use of birth control pills [5], and psychosocial factors such as low self-esteem, depression, menstrual knowledge, attitudes toward menstruation, and stress [56]. Therefore, many studies have examined the effects of interventions for discomfort caused by PMS, which focused on controlling biological and psychosocial factors [78]; however, recent reports have suggested that environmental factors exacerbated PMS symptoms [910]. An array of environmental factors play a complex role in the body, and it is difficult to determine how and when they influence people. Furthermore, symptoms and PMS onset vary between individuals, and it is difficult to eliminate the effects of other variables, all of which limit research on the topic [11].
In particular, Korean adolescents are often deprived of sufficient sleep because of academic stress, internet gaming, and smartphone use and follow an irregular sleep pattern, whereby they go to sleep late on weeknights and sleep in on weekends to compensate for this [1213]. Compared to their foreign counterparts, Korean adolescents experience more diverse types of stress, including that involving school, family, social life, finances, their looks, and friends [9]. It is therefore important to examine the correlation between stress and PMS in female students attending middle school—an age at which girls generally begin menstruation and puberty—to present foundational data for the development of PMS relief strategies.
Furthermore, individuals' thoughts and attitudes are known to influence physical symptoms [14]. A previous study [5] reported that students with strong negative attitudes toward menstruation experienced more severe menstrual symptoms, relative to those observed in students with positive attitudes.
In addition to physical and psychosocial factors that affect PMS, environmental factors, such as fine dust and endocrine disrupting chemicals (EDCs), have been identified in a number of studies worldwide [11516]. Also, various chemicals synthesized to promote convenience for humans, which are known as environmental hormones, disrupt the endocrine system. EDCs are chemicals in environmental substances or within the environment; they enter the human body and have similar actions to those of endogenous hormones, thereby blocking normal hormonal action and interfering with the synthesis, transport, metabolism, and excretion of hormones. EDCs are not broken down easily and tend to accumulate in fat and tissue in the body [16], which results in a grave impact on growth during puberty [11]. However, few studies have examined the extent of behavior that reduces EDCs exposure or explored its association with PMS in female students attending middle school.
The study aimed to examine the effects of sleep pattern, stress, attitudes toward menstruation, and behavior that reduces EDCs exposure on PMS in female students attending middle school in order to provide foundational data for developing health educational strategies for PMS interventions. The specific objectives were as follows:
1. Examine the participants' general characteristics, menstruation-related characteristics, PMS, sleep pattern, stress levels, attitudes toward menstruation, and behavior that reduces EDCs exposure.
2. Identify differences in PMS according to participants' general and menstruation-related characteristics.
3. Examine correlations between PMS and sleep pattern, stress levels, attitudes toward menstruation, and behavior that reduces EDCs exposure.
4. Identify the factors that affect PMS.
METHODS
1. Study design
The study was a descriptive correlational study and examined the effects of sleep pattern, stress, attitudes toward menstruation, and behavior that reduces EDCs exposure on PMS in female adolescent.
2. Participants
Female students (grades 1st–3nd) attending a middle school in K city were recruited. The inclusion criteria were as follows: middle school attendance, menstruation, the completion of a written consent form by legal guardians, and the provision of informed consent to participate in the study. The sample size was calculated using G*power 3.1.9 software. The minimum sample size required for multiple regression analysis was 183 with statistical significance of α=.05, power of 1-β=.90, an effect size of 0.15, and 18 predictors [17]. Considering the dropout rate, questionnaires were distributed to 200 female middle school students; of these, 198 were retrieved, and 192 were included in the final analysis, with the exception of 6 questionnaires with unanswered questions.
3. Ethical considerations
The study was approved by the institutional review board at G University (GIRB-A18-Y-005). The survey was administered only to participants from whom we had received a written informed consent form from legal guardians and personal informed consent. Further, we explained that confidentiality would be ensured, no personally identifiable information would be exposed, all data would be used only for research purposes, and participants could withdraw their consent to participate at any time.
4. Instruments
1) Sleep pattern
Sleep pattern was measured using the Korean version of the Composite Scale (KtCS) morning-, intermediate-, and evening-type developed by Yoon et al. [18]. In this 13-item scale, three items are measured using a 5-point scale (1 to 5), and 10 items are measured using a 4-point scale (1 to 4). All items use different ranges of a 4- and 5-point scale such as the different sleep time for best feeling during daytime, length of sleep, and “1 = not at all” to “4 = very” for easiness, alertness, and tiredness Total scores range from 13 to 55. Scores of ≥41 represent the morning-type pattern, scores of ≤26 represent the evening-type pattern, and scores of 27–40 represent the intermediate-type pattern. Lower scores indicate delayed sleep. Reliability was established using Cronbach's α, which were .78 at the time of scale development and .71 in the current study.
2) Stress
Stress was measured using a scale developed by Hong [9]. The scale consists of 27 items: seven pertain to grade, homework, and college admission stress; seven pertain to family stress; four pertain to stress regarding looks; three pertain to socioeconomic stress (e.g., household income and insufficient allowance), and six pertain to stress regarding peer relationships. Items are measured using a 4-point scale ranging from 1 (not at all) to 4 (always true), and total scores range from 27 to 108. Higher scores indicate higher stress levels. Reliability was established using Cronbach's α, which were .91 at the time of scale development and .90 in the current study.
3) Attitudes toward menstruation
Attitudes toward menstruation were measured using the Attitude about Menstruation Scale (AMS) developed by Yang and Youn [19] which was modified for use in the current study. In the 21-item scale, items are measured using a 7-point scale ranging from 1 (not at all) to 7 (absolutely true), and total scores range from 21 to 147. Higher scores indicate attitudes of a more negative nature toward menstruation. Reliability was established using Cronbach's α, which were .83 at the time of scale development and .79 in the current study.
4) Behavior that reduces EDCs exposure
Behavior that reduces EDCs exposure was measured using a scale developed by Kang and Lee [20] and modified for use in the current study. In the 17-item scale, items are measured using a 5-point scale ranging from 1 (very true) to 5 (not at all), and total scores range from 17 to 85. Higher scores indicate greater frequency of the occurrence of behavior that reduces EDCs exposure. Reliability was established using Cronbach's α, which were .90 at the time of scale development and .70 in the current study.
5) PMS
PMS was measured using the Shortened Premenstrual Assessment Form (SPAF) developed by Allen et al. [21] and adopted by Lee et al. [22] In the 10-item scale, items were measured using a 6-point scale ranging from 1 for (no change) to 6 (very severe), and total scores range from 10 to 60. Higher scores indicate more severe PMS, and scores of ≥27 represent premenstrual dysphoric disorder (PMDD). Reliability was established using Cronbach's α, which were .95 at the time of scale development, .90 in the study conducted by Lee et al. [22], and .92 in the current study.
5. Data collection
Data were collected from December 11 to 30, 2018. Two hundred female students (grades 1st–3rd) attending a middle school in K city were recruited via convenience sampling. Survey completion took approximately 20 minutes, and surveys were retrieved from participants immediately after completion. Participants received a pen and drink as small gifts for participation.
6. Data analysis
The data were analyzed using SPSS 21 (IBM Corp., Armonk, NY, USA). WIN. General characteristics, menstruation-related characteristics, sleep pattern, stress, attitudes toward menstruation, behavior that reduces EDCs exposure, and PMS severity were analyzed via descriptive statistics, and differences in PMS according to general and menstruation-related characteristics were analyzed using independent t-test and one-way ANOVA, with Scheffé test performed post hoc. Correlations between sleep pattern, stress levels, attitudes toward menstruation, behavior that reduces EDCs exposure, and PMS were analyzed via Pearson's correlation coefficients, and the factors that affected PMS were analyzed using multiple regression.
RESULTS
1. Participants' general and menstruation-related characteristics
Participants' mean age was 13.9 years. In total, 66 participants were in the first grade (34.4%), 66 were in the second grade (34.4%), and 60 were in the third grade (31.2%). One hundred forty-eight students (77.1%) were nonreligious. 120 (62.5%) participants were normal weight, and 45 (23.4%) were underweight. In addition, 85 participants (44.3%) exercised for more than 30 minutes at least 3 times per week, while 107 (55.7%) did not (Table 1).
Table 1
Different in General and Menstruation Related Characteristics of PMS (N=192)

Participants' mean age at menarche was 11.8 years. Regarding the length of the menstrual cycle, 85 (44.3%) participants had a 21–28-day cycle, while 63 (32.8%) had a 29–35-day cycle. Of them, 138 (71.9%) participants reported a normal amount of menstrual blood. A total of 34.4% of the students answered their menstrual pain with a score of 7–10. Among the participants, 78 (40.6%) of them stated that they used analgesics during their periods, while 114 (59.4%) did not. Furthermore, 54 participants (28.1%) reported a family history of PMS, while 138 (71.9%) did not (Table 1).
2. Participants' sleep pattern, stress, attitudes toward menstruation, behavior that reduces EDCs exposure, and PMS
In total, 9 (4.7%), 152 (79.2%), and 31 (16.1%) students had morning-, intermediate-, and evening-type sleep pattern. Lower scores indicate delayed sleep, and the mean with standard deviation of sleep score was 31.50±5.46 out of 55 (Table 2).
Table 2
Degree of Sleep Pattern, Stress, Attitudes toward Menstruation, Behavior That Reduces EDCs Exposure and PMS (N=192)
The mean scores for school related stress were highest (1.90±0.60), followed by those for stress regarding family (1.75±0.60) and appearance (1.75±0.66). Scores for stress regarding friend relationships were lowest (1.21±0.38), and the mean stress score was 44.21±11.42 out of 108 (Table 2). The mean score for attitudes toward menstruation were 72.33±14.67 out of 147. The mean score for behavior that reduces EDCs exposure was 56.57±7.65 out of 85. The mean scores for PMS were 25.30±12.28 out of 60 for the non-PMDD (n=118, 61.5%) and PMDD (n=74, 38.5%) groups (Table 2).
3. Differences in PMS according to general and menstruation-related characteristics
There were significant differences in PMS according to the length of the menstrual cycle (F=3.49, p=.017), the amount of menstrual bleeding (F=7.26, p=.001), the severity of menstrual pain (F=37.19, p<.001), use of analgesics during menstruation (t=−6.09, p<.001), and a family history of PMS (t=4.23, p<.001). PMS was more severe when the length of the menstrual cycle was <21 days or 21–28 days long, relative to that observed when it was ≥36 days. Further, PMS was more severe in girls with heavy menstrual bleeding, relative to that observed in girls with normal menstrual bleeding. PMS was most severe for those with menstrual pain scores of 7–10, followed by those of 4–6 and 0–3. In addition, PMS was more severe for those who used analgesics during menstruation and those who reported a family history of PMS (Table 1).
4. Correlations between sleep pattern, stress, attitudes toward menstruation, behavior that reduces EDCs exposure, and PMS
PMS was significantly negatively correlated with sleep pattern (r=−.15, p=.037) and behavior that reduces EDCs exposure (r=−.26, p<.001) but was positively correlated with stress (r=.24, p=.001). In other words, girls experienced more severe PMS with lower amounts of sleep, less frequent occurrence of behavior that reduces EDCs exposure, and higher levels of stress (Table 3).
Table 3
Correlation of Variables (N=192)

5. Factors affecting PMS
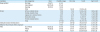
The results of the multiple regression analysis to determine factors affecting PMS, with variables confirmed in the univariate analysis (i.e., menstrual cycle, amount of menstrual bleeding, use of analgesics during menstruation, menstrual pain, family history of PMS, sleep pattern, stress, and behavior that reduces EDCs exposure) as independent variables. The results showed that severity of menstrual pain (β=.28), use of analgesics during menstruation (β=.17), family history of PMS (β=−.16), stress (β=.19), and behavior that reduces EDCs exposure (β=−.17) exerted significant effects on PMS. The data met the assumption of normality and equality of variance, and multicollinearity was not an issue, with tolerance of 0.615–0.878 and a variation inflation factor of 1.138–1.626. The regression model for PMS was significant (F=15.48, p<.001), and these variables explained 37% of the total variance (Table 4).
Table 4
Factors Influencing PMS (N=192)

DISCUSSION
This study aimed to examine the relationships between sleep pattern, stress, attitudes toward menstruation, and behaviors that reduces EDCs exposure in Korean girls attending middle school and factors that affect PMS. Participants' mean age was 13.9 years, and their mean age at menarche was 11.8 years, which was similar to that observed in a previous study [23]. The most common length of the menstrual cycle, which differed significantly according to PMS, was 21–28 days (44.3%), followed by 29–35 days (32.8%), and <21 days (13.5%). These were similar to cycles reported in a previous study [24] and PMS severity increased with decreasing cycle length. Approximately 71.9% of participants reported normal menstrual bleeding, while 22.9% reported heavy menstrual bleeding, and girls with heavy bleeding experienced more severe PMS. These results were similar to those of some previous studies [25] but contradictory to those of other studies that reported that PMS was more severe in girls with light or normal menstrual bleeding [12]. Further, PMS was more severe in girls with a family history of PMS, as shown in a previous study [5]. Approximately 59.9% of the girls reported moderate-to-severe menstrual pain; this proportion was slightly higher relative to that of girls attending middle school who experienced moderate-to-severe pain (50.6%) in a recent study [26]. Because more than half of girls attending middle school experience moderate-to-severe PMS, relevant interventions should be developed and administered.
Similar to the findings of a previous study involving high school students [27], sleep quality was moderate, with 79.2% of participants showing the intermediate-type of sleep pattern and a mean score of 31.5 (range: 13–55). However, Korean adolescents begin school earlier each day and sleep later at night as they advance in grade, relative to their foreign counterparts [13], and they are likely to lack sufficient sleep and experience poor sleep quality.
Unlike adolescents in other countries, Korean adolescents were most stressed by school grades, homework, and college admission. These were followed by family stress and stress regarding their looks. These results were similar to those of previous findings involving high school girls [9]. Fierce competition for college admission and rampant obsession with appearance induces severe stress in Korean adolescents, necessitating programs that relieve these factors. Thus, the specific programs are needed to reduce the study related stress for adolescents with severe PMS.
The mean score for behavior that reduces EDCs exposure was 56.5, which was high, as in previous studies [20]. However, a previous study examining awareness of and behavior related to EDCs in Korean students attending middle school [10] reported that the students obtained information regarding EDCs from the public media and perceived them as hazardous substances. Moreover, students with higher grades possessed greater knowledge concerning EDCs, relative to that of students with lower grades, and behavior that reduces EDCs exposure was strongly correlated with knowledge scores. Therefore, it is necessary to develop intervention programs to engage students' behaviors that reduces EDCs exposure by providing accurate knowledge for PMS prevention.
The mean PMS score was 25.30 (range: 10–60). Approximately 38.5% of participants were in the PMDD group, for which the mean PMS score was 38.39, which was similar to that shown in a previous Korean study [12]. PMDD is often neglected because its origin is uncertain and treatment is challenging. However, relevant education and support should be provided to prevent progression to PMDD and reduce discomfort.
In the current study, menstrual pain, use of analgesics during menstruation, a family history of PMS, stress levels, and behavior that reduces EDCs exposure influenced PMS. In a study involving 1,688 Korean high school girls [5], those with menstrual pain and a family history of PMS experienced PMS more frequently relative to other girls. In addition, a study involving female college students and adults [28] reported that menstrual pain and family history affected PMS, as in the current study. The association between menstrual pain and PMS has been documented extensively in the literature; therefore, effective PMS management could reduce the adverse effects of menstrual pain and discomfort on school works and daily lives in girls attending middle school. Further, as girls with a family history of PMS experienced more severe PMS, relative to those without such a history, schools should provide special management for students with this family history. A study involving 1,087 Korean students attending middle and high school [25] and a study involving female college students and adults showed that stress influenced PMS [28]. Therefore, PMS interventions for girls attending middle school should be designed in reflection of the different stressors involved. Behavior that reduces EDCs exposure also influenced PMS; this finding was similar to those of a study involving female Korean college students [27]. EDCs vary widely in type and mechanism, and although prenatal exposure to EDCs was reported to exert a strong impact in foreign studies, studies examining the association between EDCs exposure and PMS are scarce. Further, studies examining factors related to EDCs are required in Korea, and researchers should explore the relationship between PMS and EDCs in large, diverse samples. In the current study, PMS severity increased as stress levels increased and the occurrence of behavior that reduces EDCs exposure decreased. Therefore, intervention programs that reduce PMS in Korean girls attending middle school are required.
The current study was meaningful, in that it presented the association between PMS and behavior that reduces EDCs exposure in Korean girls attending middle school. However, the findings could not be generalized to other groups, as the sample consisted of girls attending a middle school in a single region, and future studies should recruit more diverse samples to identify the factors that affect PMS including behavior that reduces EDCs exposure. Furthermore, numerous scales that measure behavior related to EDCs exposure were developed for use with adults; therefore, tools that are appropriate for adolescents should be developed. Moreover, based on these findings, additional studies should be required to develop intervention programs that reduce stress and behavior that EDCs exposure in Korean girls attending middle school.
CONCLUSION
This was a descriptive correlational study that aimed to examine the effects of sleep pattern, stress, attitudes toward menstruation, and behavior that reduces EDCs exposure on PMS in female students attending middle school. The results showed that severity of menstrual pain exerted the strongest effect on PMS, followed by use of analgesics during menstruation, a family history of PMS, stress, and behavior that reduces EDCs exposure. These variables explained 37% of the total variance. Based on the findings, we recommend that health intervention program is developed to prevent PMS for adolescents including educational information and activities for managing their stress and promoting the behaviors that reduces EDCs exposure.
 XML Download
XML Download