

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Some strain of Clostridium difficile isolates produce the binary toxin, C. difficile transferase (CDTa) in addition to pathogenic toxins like toxin A and toxin B. About 6-12.5% of isolates produce binary toxin. Since 2002 in North America and Europe, the proportion of binary toxin-producing strains has increased to 30-65% of all isolates [1, 2]. In Korea, the proportion of isolated binary toxin-producing strains is low with 4-7%, even after 2009 when these hypervirulent binary toxin strains were first reported [3, 4].
The pathogenicity of binary toxin is not clear yet. Binary toxin is an ADP-ribosylating toxin which disaggregates actin cytoskeleton, and induces effusion in intestinal epithelial cell cultures and changes the cells to a round shape which in turn causes apoptosis [5]. However, when binary toxin was given to hamsters, the colonization of the isolates occurred in 70-80% of the hamsters but they did not manifest diarrhea or expire [6]. From a recent report, binary toxin plays an important role in the immediate colonization of C. difficile by creating a thin microtubule in the surface of intestinal epithelial cells to assist in the easy adherence of C. difficile onto the surface of intestinal cells [7].
There are various ribotype strains which produce binary toxin. The hypervirulent strain, BI/NAP1/027 is a prevalent strain in North America and is known to significantly increase morbidity and mortality in infected patients compared to other stains [8]. In addition to the production of binary toxin, variations in tcdC, which is the regulatory gene of toxin A and toxin B, increases its virulence with an increase in the production and duration of the toxin [9]. This epidemic strain is resistant to fluoroquinolone; hence, the recent increase in the use of respiratory fluoroquinolone is expected to be an important selection pressure [10].
Recently, there was a case of the BI/NAP1/027 strain in Korea [11], but there are no data on the binary toxin-producing strain in general. Therefore, the authors conducted this study to find out the general current circumstances of binary toxin-producing C. difficile infection (CDI) in Korea. In this study, the clinical manifestations and risk factors for acquisition of binary toxin-producing CDI was compared to toxin A and B positive strain infections. Moreover, the distribution of PCR ribotypes in binary toxin-producing strains in Korea was identified along with the major results of antimicrobial susceptibility tests.
Materials and Methods
1. Study subjects
The study subjects were patients 18 years or older who were diagnosed as CDI with cultivated C. difficile in stool cultures and admitted to Hanyang University Seoul Hospital from September 2008 to January 2010. The toxin producing genes from the C. difficile isolates were confirmed and the patients were divided according to presence of binary toxin gene. The control group (A+B+CDT- group) included patients infected with a toxin A-positive, toxin B-positive, binary toxin-negative strain, and the patient group (A+B+CDT+ group) included patients infected with a toxin A-positive, toxin B-positive, binary toxin-positive strain. This study was approved by the institutional review board of Hanyang University Hospital (HYUH IRB 2010-R-12). Informed consent was waived by the board.
2. Diagnosis related definitions and data collection
A diagnosis of CDI was made in the following cases: C. difficile toxin A&B assay (VIDAS® C. difficile toxin A&B; BioMerieux SA, Marcy I'Etoile, France) positive in patients who complained of unformed stools 3 times daily or for more than 2 days or longer, otherwise 6 times or more within 36 hours; the confirmation of toxin producing genes from the isolated C. difficile in stool cultures; or psuedomembranes on the endoscopy or biopsy [12].
Age, sex, length of stay in the hospital, underlying disease including Charlson's score, and catheter utilization were collected for the clinical data [13]. The admission history of the past 2 months, operation history, history of antibiotic use and the dose were collected and use of proton pump inhibitor (PPI), H2 blocker (H2B) and probiotics were checked. Amounts of antibiotics administered were calculated as the number of defined daily dose (DDD) [14]. The values for the white blood cell (WBC) level, albumin level, and C-reactive protein (CRP) at the time of diagnosis were recorded and the presence of the pseudomembrane was checked through endoscopy.
For severity assessment, a patient was over 60 years old, temperature over 38.3℃, WBC over 15,000 cells/mm3, and albumin less than 2.5 mg/dL, respectively, was given 1 point and added up. Then, severe CDI was defined as when the total points were 2 points or greater [15, 16]. For clinical outcome, success was defined as improvement in diarrhea and symptoms within 14 days of the initiation of treatment while other cases were regarded as failure [17]. Recurrence was defined as the manifestation of symptoms of CDI after the improvement of symptoms from day 10 after treatment initiation, and a global cure was defined when there was no recurrence in patients who received the initial treatment [18].
3. Microbiology tests
1) C. difficile culture
After alcohol shock treatment, stool specimen were cultivated on CDMN-TA agar (C. difficile Moxalactam-Norfloxacin-Taurocholate agar, Oxoid Ltd., Cambridge, UK) supplemented with 7% horse blood. Colonies of C. difficile were identified by Rapid ID 32A (BioMerieux SA, Marcy I'Etoile, France).
2) Multiplex PCR
To identify toxin genes, multiplex PCR was performed with template DNA. After electrophoresis of the amplified products, toxin genes (tcdA, tcdB, cdtA, and cdtB) were defined according to band size [19].
3) PCR ribotyping of C. difficile strains
With minor modifications, PCR ribotyping was performed as described elsewhere [3]. After electrophoresis of the PCR products, the pattern was checked visually. Ribotype 027 (BI/NAP1/027), ATCC 43598 (ribotype 017) and standard strains from the ECDC-Brazier collection were used for the reference [3].
4) Antimicrobial susceptibility test
Antimicrobial susceptibility tests for the subject strains were conducted with the following antibiotics: clindamycin, moxifloxacin, vancomycin, metronidazole, piperacillin-tazobactam and rifaximin [20]. Breakpoints for each antimicrobial agent were defined by CLSI guideline. C. difficile ATCC 700057 served as a quality control strain.
4. Statistical analysis
SPSS 18.0 version (SPSS, Chicago, IL, USA) was used for statistical analysis. Pearson's Chi-square test or Fisher's exact test was used for the analysis of categorical variables, and independent t-test or Mann-Whitney U-test was used for the analysis of continuous variables. Multiple logistic regressions were performed to identify risk factors for acquisition of binary toxin producing strains and clinical difference according to presence of binary toxin gene. A P-value of < 0.05 by two-tailed test was considered statistically significant.
Results
1. Clinical Characteristics
One hundred and five cases of A+B+CDT- groups and 11 cases of A+B+CDT+ groups were identified during the study, and the clinical characteristics were compared and analyzed between the 2 groups.
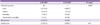
1) Comparisons of demographic characteristics and risk factors (Table 1)
Patient age, sex, underlying disease and operation history and the length of stay in hospital were similar between two groups. From the previous medication history, PPI and probiotics were administered more frequently in the A+B+CDT- group, but there was no statistically significant difference. According to classes of antimicrobial agents, the glycopeptide class was administered more frequently (19.0% vs 45.5%, P = 0.057) and in higher doses (P = 0.042) in the A+B+CDT+ group. Clindamycin was administered more frequently in the A+B+CDT+ group, but there was no statically significant difference (P = 0.069).
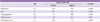
2) Comparisons of clinical features (Table 2)
The severity of CDI between the 2 groups was compared (Table 2). The incidence of leukocytosis was higher in the A+B+CDT+ group (36.4% vs. 13.3%)but there was no statistically significant difference in WBC counts (P = 0.067). Percentage (%) of old age, fever, and hypoalbuminemia also were not different between groups. The incidence of severe CDI was 36.4% and 19.0% in the A+B+CDT+ group and A+B+CDT- group, respectively, but there was no statically significant difference. Propertional pattients with mucoid stool was greater in the A+B+CDT+ group with statistical significance (18.1% vs. 54.5%, P = 0.012). However, there was no significant difference between the 2 groups in stool frequency, abdominal pain, and tenderness. There were no significant differences between the 2 groups in albumin values and CRP. The confirmed cases of pseudomembranous colitis among the patients who had endoscopy done were 38.5% (10/26) and 50.0% (1/2) in the A+B+CDT- group and A+B+CDT+ group, respectively, in which the A+B+CDT+ group had an odds ratio of 1.6 relative to the A+B+CDT- group (95% Confidence Interval (CI: 0.1 to 28. 6).
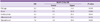
3) Clinical outcome (Table 3)
There was no difference in the proportion of treated patients (65.7% in the A+B+CDT- group vs. 63.6% in the A+B+CDT+ group, P > 0.99). As the initial drug for treatment, 86.8% of CDI patients were received metronidazole. There was no difference between the 2 groups for the initial drug used in the treatment (87.0% in the A+B+CDT- group vs. 85.7% in the A+B+CDT+ group, P > 0.99). From a comparison of the mortality rate and attributable mortality rate, the mortality rate was 10.1% and the attributable mortality rate was 1.4% in the A+B+CDT- group, and there were no cases of death in the A+B+CDT+ group; however, there was no statistical difference. Recurrence was lower in the A+B+CDT+ group (0% vs. 21.7%), and global cure was higher in the A+B+CDT+ group (85.7% vs. 62.3%), but both results did not have any statistically significant differences.
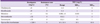
4) Analysis of risk factors and predictable factors in the acquisition of binary toxin producing strains (Table 4)
To evaluate the risk factor associated with previous medication within 2 months for binary toxin producing CDI, multiple logistic regressions were performed. In this model, Charlson's score was adjusted for the risk of medication use due to severe underlying disease. The use of glycopeptides and the risk of A+B+CDT+ strain acquisition were statistically significant (OR: 6.2, 95% CI: 1.4 to 28.6, P = 0.019). There was a correlation with the use of clindamycin and A+B+CDT+ strain acquisition, but it was not statistically significant (OR: 4.6, 95% CI: 1.0 to 22. 3, P = 0.057), and the use of probiotics showed a statistically significant inhibitory effect on the acquisition of the A+B+CDT+ strain (OR: 0.1, 95% CI: 0.0 to 0.8, P = 0.026).
To determine whether the clinical findings or laboratory findings at the time of diagnosis can predict CDI caused by binary toxin-producing strains, multiple logistic regressions were performed. Age, fever, leukocytosis and albumin level, as well as cases with mucoid stool which showed a significant difference in cross tabulation analysis were included. The odds ratio of leukocytosis and mucoid stool in binary toxin-producing CDI was 5.2 times (95% CI: 1.1 to 25.4, P = 0.043) and 7.6 times (95% CI: 1.6 to 35.6, P = 0.010), respectively (Table 5).
2. Microbiological characteristics
1) PCR ribotype distribution of binary toxin-producing C. difficile strains
The PCR ribotypes of a total of 11 binary toxin-producing strains were identified. A total of 5 types of PCR ribotypes were identified with 4 strains of ribotype 130, 3 strains of ribotype 027, 1 strain of ribotype 267, and 1 strain of ribotype 122 were identified. Two strains had a new PCR ribotype which is not listed on the ECDC-Brazier collection, and they were classified as C1 according to the classification by Kim et al. [4].
2) Antimicrobial susceptibility of binary toxin-producing strains
The antimicrobial susceptibility of the 11 A+B+CDT+ and A+B+CDT- strains was compared (Table 6) [20]. The A+B+CDT- strains had a high resistance rate for clindamycin and moxifloxacin, 69% and 63%, respectively, but the A+B+CDT+ strains were susceptible to both clindamycin and moxifloxacin. One case out of the 11 A+B+CDT+ strains manifested resistance to rifaximin with the patient from which the isolate was from having no history of rifaximin use; hence, the resistance rate was 9.1%.
Discussion
There has been a remarkable increase in the binary toxin-producing BI/NAP1/027 strain in North America since 2002. On the other hand, binary toxin-producing strains have been identified sporadically in Korea. Data on the features of infections, distribution of PCR ribotypes, and antimicrobial susceptibility tests for binary toxin-producing CDI other than 027 strains are not available [21]. Therefore, the authors investigated the clinical impact and microbiologic characteristics of binary toxin-producing strains isolated from a hospital. Binary toxin-producing strains in Korea showed various ribotypes including the 027 strain, and the proportion of the BI/NAP1/027 strain among the entire binary toxin-producing strains was 15-27% and 5% among the entire C. difficile strains.
Generally in North America and Europe, the frequency of the BI/NAP1/027 strain among binary toxin-producing strains varies from 20-80%, and includes 30-60% of all C. difficile strains [22, 23]. The increase in those binary toxin-producing strains was determined as the major cause of the increase in the CDI incidence since 2002 [9].
The epidemic BI/NAP1/027 strain shows a resistant pattern against respiratory fluoroquinolones such as moxifloxacin, and recently, the resistant 027 strain is increasing due to selective pressure with the increase in use of those medications [10]. In this respect, there was a report on the epidemics of ribotype 018 and 017 in Korea correlated with the high resistant rate to moxifloxacin and clindamycin [3]. However, binary toxin-producing strains in this study were highly susceptible to antimicrobial agents and could not have survival benefits in a hospital environment. This would be the reason for the low incidence of binary toxin-producing strains in hospitals in Korea. Ribotype 027 in Korea, which is highly susceptible to antimicrobials, was presumed to be a historical strain that is different to the recent epidemic strains. However, from a recent study, resistance to moxifloxacin was observed in the 027 strain in Korea (6/7, 85%); hence, the possibility of an increase in CDI incidence or outbreak in the future should be considered [21].
Infection due to binary toxin-producing strains is known to have higher mortality relative to binary toxin-negative strain infections, and increases the mortality and attributable mortality [24, 25]. In infections due to binary toxin-producing strains, abdominal pain and diarrhea were more severe [24], the incidence of severe CDI more frequent, and mortality 2.5 times higher [25]. Some contradicting reports have been published [26], but mortality from infection due to binary toxin-producing strains would be markedly high because the mortality rate of CDI due to the historical strains was 3.0-3.5% and the CDI mortality rate in Canada and the United States where binary toxin-producing strains are endemic is 13-14% [27-29]. Bacci et al. investigated the 30-day mortality by comparing 193 cases of PCR ribotype 027 and 72 cases of other ribotypes among the binary toxin-producing strains to 212 infection cases of the A+B+CDT- strain, and as a result, the additional mortality from the infection due to the binary toxin-producing strains was up to 60%, regardless of the ribotype (OR: 1.60, 95% CI: 1.0 to 2.4) [23]. In this study, the frequency of leukocytosis and mucoid stool were high in binary toxin-producing CDI. However, the overall incidence of severe CDI was not different between the 2 groups and there was no difference in mortality.
The use of glycopeptides was a significant risk factors for infection by binary toxin-producing strains. However, the strains in both of the groups showed sensitivity to vancomycin and the vancomycin MIC50 of binary toxin-producing strains was 0.5 mg/L which was lower than the MIC50 of the A+B+CDT- strain with 1 mg/L. From amicrobiological perspective, vancomycin is not considered to be a medication which causes selective pressure in binary toxin-producing strains; however, more cases are warranted to further verify this in the future.
There were limitations in this study. It was difficult to obtain statistical significance because only 11 cases of infection due to binary toxin-producing strains occurred during 17 months. In addition, the data were from a single center limiting its applicability to the general population in Korea. Therefore, further studies are warranted in which data are collected from a number of centers.
In conclusion, binary toxin-producing strains in Korea are not common, presenting various PCR ribotypes and are susceptible to various antimicrobial agents. Clinically, the incidence of leukocytosis and mucoid stool were more frequent in binary toxin-producing CDI, but there was no remarkable difference in the mortality rate. The risk factor for binary toxin-producing CDI in Korea was the use of glycopeptides.


 XML Download
XML Download