

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
A 35-year-old man with known coccidioidal meningitis developed a severe headache and vomiting during routine treatment. Hydrocephalus was visible on brain imaging, and CSF study revealed pleocytosis, lowering of glucose, and increased intracranial pressure. Dexamethasone and mannitol was used for intracranial pressure control. Intrathecal amphotericin B administration and switching to itraconazole resulted in gradual improvement of symptoms. After 4 months of discontinuing amphotericin B intrathecal administration, the patient developed severe headaches with vomiting, diplopia and tandem gait. Coccidioidal meningitis aggravation was suspected based on brain MRI and CSF studies. Ventriculo-peritoneal shunt insertion was performed for intracranial pressure control and the combined therapy of intrathecal amphotericin B administration and fluconazole was maintained. This combined regimen kept the meningitis stable for 1 month.
Figures and Tables
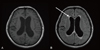
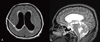
Figure 1
Diffuse dilatation of all ventricles with peri-ventricular high signals was noticed on brain MRI.

References
1. Johnson RH, Einstein HE. Coccidioidal meningitis. Clin Infect Dis. 2006. 42:103–107.

2. Pérez JA Jr, Johnson RH, Caldwell JW, Arsura EL, Nemecheck P. Fluconazole therapy in coccidioidal meningitis maintained with intrathecal amphotericin B. Arch Intern Med. 1995. 155:1665–1668.
3. Drake KW, Adam RD. Coccidioidal meningitis and brain abscesses: analysis of 71 cases at a referral center. Neurology. 2009. 73:1780–1786.
4. Ampel NM. Coccidioidomycosis: a review of recent advances. Clin Chest Med. 2009. 30:241–251.
5. Kim YG, Shin KC, Lee SS, Moon MS. The clinical consideration for spinal epidural abscess. J Korean Neurosurg Soc. 1976. 5:87–92.
6. Baek JH, Park EY, Jung YS, Hong JW, Chae Y, Jin SJ, Choi HK, Shin SY, Han SH, Chin BS, Kim CO, Choi JY, Song YG, Cho NH, Kim JM. Recurrent coccidioidomycosis manifesting as osteomyelitis in Korea. Infect Chemother. 2009. 41:253–257.
7. Kim YJ, Cho HM, Kim JH, Kim IH, Shin C, Son SW. Disseminated coccidioidomycosis with cutaneous manifestation. Korean J Dermatol. 2005. 43:1379–1382.
8. Chang S, Shim SH, Kwak JE, Joo M, Kim H, Park HJ, Kwak YG, Chi JG. A case report of cutaneous coccidioidomycosis. Korean J Pathol. 2008. 42:223–225.
9. Park JC, Kim JH, Ku NS, Lee KH, Choi YK, Lee YH, Kim YK, Kim MS, Song YG, Shin SY, Kim YA, Park YS, Cho SH, Kim CK, Yong D, Choi JY, Kim JM. A case of disseminated coccidioidomycosis with pelvic bone and paravertebral abscess. Infect Chemother. 2006. 38:296–299.
10. Park DJ, Jang YH, Lee SJ, Na GY, Kim DW, Kim SW. A case of coccidioidomycosis showing cutaneous and pulmonary nodules. Korean J Med Mycol. 2004. 9:190–195.
11. Kim SW, Oh JY, Kim EJ, Park GM. Pulmonary coccidioidomycosis in immunocompetent patient. Tuberc Respir Dis. 2009. 66:220–224.
12. Stevens DA, Shatsky SA. Intrathecal amphotericin in the management of coccidioidal meningitis. Semin Respir Infect. 2001. 16:263–269.
13. Cortez KJ, Walsh TJ, Bennett JE. Successful treatment of coccidioidal meningitis with voriconazole. Clin Infect Dis. 2003. 36:1619–1622.
14. Proia LA, Tenorio AR. Successful use of voriconazole for treatment of Coccidioides meningitis. Antimicrob Agents Chemother. 2004. 48:2341.
15. Davis LE, Cook G, Costerton JW. Biofilm on ventriculo-peritoneal shunt tubing as a cause of treatment failure in coccidioidal meningitis. Emerg Infect Dis. 2002. 8:376–379.
16. Kriesel JD, Sutton DA, Schulman S, Fothergill AW, Rinaldi MG. Persistent pulmonary infection with an azole-resistant coccidioides species. Med Mycol. 2008. 46:607–610.
17. Thompson GR 3rd, Lunetta JM, Johnson SM, Taylor S, Bays D, Cohen SH, Pappagianis D. Early treatment with fluconazole may abrogate the development of IgG antibodies in coccidioidomycosis. Clin Infect Dis. 2011. 53:e20–e24.
 XML Download
XML Download