

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In South Korea, health check-ups for screening purposes have recently become quite popular. Due to a high incidence of gastric cancer, esophagogastroduodenoscopy (EGD) is offered biannually in individuals older than 40 years via Korea's National Health Insurance check-up program.
The prevalence of gastroesophageal reflux disease in Asia has increased. Prior to 2000, the prevalence of reflux esophagitis diagnosed on EGD was less than 10%,1 and since then, has gradually increased up to 13.8%.23 In a national study in Korea from 2005 to 2008, the prevalence of reflux esophagitis was reported as 7.91% based on endoscopic findings at health check-ups (n=25536).4
Use of sedated EGD has increased to control patient anxiety and pain during EGD. Commonly, patients are allowed to opt for sedation if it is not contraindicated, since sedation improves patient tolerance during the procedure. Many studies have been published about sedation regimens during EGD, as well as associated risks and benefits, with appropriate safety measures and monitoring practices.56 While EGD can be performed correctly under sedation, patients may not be able to perform deep inspiration when examining the esophagogastric junction (EGJ). Thus, sedation likely affects the diagnosis of gastroesophageal reflux-related findings. The EGJ is functionally and anatomically complex and is not easily evaluated. Although the methods, degrees, and duration of sedated EGD have been studied extensively, there have been no reports on the influence of sedation on diagnosis of disease during EGD. Therefore, we elected to study the implications of sedation on the diagnosis of upper gastrointestinal disease, particularly gastroesophageal reflux-related findings, during EGD.
MATERIALS AND METHODS
Patients
We performed a retrospective review of data from 28914 patients older than 20 years who underwent EGD at the Severance Hospital, Yonsei University College of Medicine, in Seoul, Korea from January 2011 to December 2011. A total of 28914 patients received an EGD during the study period. We excluded therapeutic EGD, such as endoscopic mucosal resection, endoscopic submucosal dissection, percutaneous endoscopic gastrostomy, and hemostasis for gastrointestinal bleeding; emergency EGD; and scheduled EGD after upper gastrointestinal malignancy treatment. Consequently, the study population comprised 18546 patients who received a diagnostic EGD and fulfilled the inclusion criteria. Of these, 10471 patients (56.4%) underwent non-sedated EGD and 8075 patients (43.5%) underwent sedated EGD (Fig. 1). Data related to the patient's characteristics and endoscopic findings were extracted.
Esophagogastroduodenoscopy
EGD was performed by experienced endoscopists who had each performed more than 3000 upper endoscopies and well-trained endoscopists who performed at least more than 130 cases, which are minimum quality requirements for competence according to a specialist medical society.7
EGD was accomplished in the left lateral decubitus position, and patients received topical pharyngeal anesthesia with lidocaine spray. All patients were assessed with a history and physical examination prior to administering sedation to identify factors that may increase the risk of an adverse outcome. The sedated EGD was performed by low-dose propofol sedation. Before initiation of EGD, a 20 gauge (1.0 mm) i.v. cannula was placed in the patient's forearm for propofol injection. An additional 20 mg of propofol was injected if the target level was not obtained.6 Low-dose propofol was administered for endoscopic sedation by nurses supervised by the endoscopists. Both the endoscopists and nurses had basic cardiac life support certification.8 The target level of sedation was conscious sedation that maintained both ventilator and cardiovascular function, and allowed patients to make a purposeful response to verbal or tactile stimulation. Patient monitoring was performed in accordance with the recommendations of the American Society for Gastrointestinal Endoscopy.6
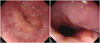
We used a gastrointestinal videoscope (GIF-Q260, GIF-H260; Olympus Optical Co. Ltd., Tokyo, Japan) with an outer diameter of 9.2, 9.8 mm by an oral approach. Endoscopic examination of the EGJ was performed using a high-definition white-light endoscope without specialized equipment, such as chromoendoscopy or narrow band imaging, and was inspected as described below. We asked the patients to hold their breathing after deep inspiration. Then, we observed the EGJ when it was most widely opened during peristalsis (Fig. 2). The remainder of the endoscopic examination was performed according to the department's standard operating procedure. The EGJ was defined to include the squamocolumnar junction, the proximal margin of gastric folds, the distal end of the palisade zone, and the location of pinchcock. Endoscopic findings of reflux esophagitis in the lower esophagus were classified according to the Los Angeles (LA) classification as grades A to D, and were based on the longest length of a mucosal break and the confluence of erosion. Six endoscopic criteria were used to define minimal change esophagitis: erythema, blurring of the Z-line, white turbid discoloration, decreased vascularity, friability, and edema or accentuation of the mucosal fold.91011
This study protocol was approved by the Institutional Review Board of Yonsei University Hospital (4-2012-0124) and the study was conducted in accordance with the Helsinki Declaration.
Statistical analysis
Continuous variables are expressed as the mean±standard deviation. The chi-square test was used to compare categorical variables, and a t-test was used to compare continuous variables. Logistic regression adjusted for age, sex, and body mass index (BMI) was used to assess the effect of sedation on the diagnosis of gastroesophageal reflux-related findings during EGD. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was conducted using SAS 9.2 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Among the 18546 patients, 9369 (50.5%) were men and 9177 (49.4%) were women. The mean age was 56 years (range: 20-96 years, SD: 13.9) and the mean BMI was 23.1 (SD: 3.4). Table 1 shows the characteristics of the study population. The data revealed significant differences in clinical characteristics, such as sex, age, BMI, hypertension, and diabetes mellitus. However, as data on smoking, alcohol, hypertension, and diabetes mellitus were missing in about half of the patients, we do not include these variables when comparing and analyzing sedation effects during EGD. We adjusted for age, sex, and BMI when evaluating the collected data.
Table 2 demonstrates the reasons for diagnostic EGD, which we classified into evaluation for symptoms and previous findings and a regular health check-up. The common purpose of diagnostic EGD was to evaluate gastrointestinal symptoms and previous EGD findings. There were no significant differences between the sedated and non-sedated groups regarding the purposes of diagnostic EGD.
Table 3 shows differences in the endoscopic findings of the EGJ observed between the sedated EGD group and non-sedated EGD group. Sedated EGD was significantly associated with less frequent detection of minimal change esophagitis [odds ratio (OR), 0.651; 95% confidence interval (CI), 0.586 to 0.722] and hiatal hernia (OR, 0.699; 95% CI, 0.564 to 0.866) at the EGJ. Likewise, other findings at the EGJ, such as reflux esophagitis of LA classification A (OR, 0.949; 95% CI, 0.807 to 1.116), B (OR, 0.782; 95% CI, 0.589 to 1.038), C (OR, 0.872; 95% CI, 0.447 to 1.700), and D (OR, 0.639; 95% CI, 0.226 to 1.805), and Barrett's esophagus (OR, 0.794; 95% CI, 0.586 to 1.076), were also less frequently detected, although the differences therein between the two groups was not significant.
Findings in the stomach, such as early gastric cancer (OR, 1.145; 95% CI, 0.995 to 1.317), advanced gastric cancer (OR, 0.896; 95% CI, 0.768 to 1.044), and gastric ulcer (OR, 0.963; 95% CI, 0.857 to 1.083), did not differ between the two groups (Table 4).
DISCUSSION
Conscious sedation is often performed in diagnostic and uncomplicated therapeutic EGD. The purpose of this study was to investigate the influence of sedation on the diagnosis of gastroesophageal reflux-related findings during EGD. After adjusting for sex, age, and BMI, diagnoses of minimal change esophagitis and hiatal hernia were more frequent for non-sedated EGD than sedated EGD (12.7% vs. 10.0% and 3.3% vs. 1.9%, respectively). Reflux esophagitis of LA classification A to D was not significantly different between the sedated and non-sedated EGD groups in this study.
There are two possible explanations for the greater detection of a minimal change esophagitis in non-sedated EGD. One reflects the sedation itself during EGD, while the other involves the effect of propofol on esophageal motility. Sedation impacts EGJ observation in the following two ways: first, sedation can provide endoscopists enough time to observe the EGJ as long as they want, compared to non-sedated EGD. Second, sedation hampers performing the procedure at the EGJ adequately due to a lack of cooperation between the endoscopist and the patient with regard to breathing, which was observed in this study.
Deep inspiration generates negative pressure in the thoracic cavity. In this interim, intraabdominal pressure increases and the diaphragm flattens.12 Thus, deep inspiration facilitates the extension of the esophagus so that the EGJ can be observed easily. This may have caused the difference in the diagnosis of the gastroesophageal reflux-related finding between the two groups in this study.
When propofol is used at a lower dose (0.3 mg/kg), there is no alteration in pressure of the lower esophageal sphincter. However, there is an increase in pressure in young patients (less than 30) after a high dose (0.9 mg/kg) of propofol. In our study, almost all patients were older than forty; therefore, propofol itself would not be expected to affect the motility of the esophagus.13
Minimal change esophagitis was defined as a whitish or reddish, edematous change and erosion that was not a mucosal break. The interobserver agreement for this lesion is low in comparison to that of reflux esophagitis LA classification A to D,14 so the diagnosis of this lesion must made more precisely and carefully. Although minimal changes are one of the endoscopic findings of non-erosive reflux disease, the clinical significance of these minimal changes is controversial. In our previous report, most endoscopic findings indicating minimal changes were not related with symptoms of gastroesophageal reflux disease. Together with previous studies about minimal change esophagitis, diagnosis of minimal change esophagitis should be reconsidered because of low interobserver agreement, as well as a lack of clinical meaning and variability in the methods of examination.
In Asia, several studies have been performed on the prevalence of endoscopy-based reflux esophagitis. The prevalence of endoscopic esophagitis is generally less than 10%, although it has been increasing in recent years.15161718 In our study, the prevalence of endoscopic reflux esophagitis was found to be 5.7%, which is similar to the 7.9% prevalence rate reported in 200517 and the 3.4% prevalence rate in 2001 for Koreans,19 although lower than the prevalence observed in the West.20 Barrett's esophagus has a very low prevalence in Asia of less than 0.03% of the general population2122 and 2% of upper gastrointestinal symptoms.3 The prevalence of Barrett's esophagus was 1.4% in this study. The reason for this relatively high prevalence was that only 21.8% of EGD was conducted as a routine health check-up, while the majority was conducted for the evaluation of upper gastrointestinal symptoms, diagnosis of disease, and after receiving a referral to our hospital. Although there was a difference (OR, 0.794; 95% CI, 0.586 to 1.076) between the sedated and non-sedated EGD groups, it was not statistically significant (p=0.136).
One of the risk factors of Barrett's esophagus is hiatal hernia. Hiatal hernia is defined as the persistent or recurrent herniation of parts of the stomach through the esophageal hiatus into the chest cavity.23 For accurate observation of a hiatal hernia, the endoscopist requires proper air inflation in the stomach and the patient's cooperation in breath control. Therefore, sedation affects the diagnosis of gastroesophageal reflux-related findings, such as minimal change esophagitis and hiatal hernia, as we found in this study.
Finally, there are several limitations in our study. Firstly, this study was performed retrospectively. Although all endoscopic data were recorded prospectively and properly selected, the chance of bias cannot be negated. Secondly, confounding factors to have a potential effect on examination of EGJ including proton pump inhibitor (PPI) medication, obesity, smoking status, and chronic airway diseases, such as chronic obstructive pulmonary disease and asthma, to cause airflow limitation were not thoroughly evaluated. This problem can be solved by future prospective studies. Thirdly, this study was performed at a tertiary referral hospital with a high prevalence of gastric cancer compared to the general population. Therefore, it is difficult to generalize our findings regarding the potential effect of sedation on diagnoses.
In this study, we have shown that sedation during the EGD can affect the sensitivity of diagnosis of minimal change esophagitis and hiatal hernia. Sedation might interfere with detailed examination of the EGJ, compared to non-sedative EGD. However, clinically significant findings such as reflux esophagitis of LA classification A to D and Barrett's esophagus were not influenced by sedation. Therefore, we suggest that patient's sedation status should be considered while evaluating minimal change esophagitis or hiatal hernia.





 XML Download
XML Download