

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Attention-deficit/hyperactivity disorder (ADHD) is a common neuropsychiatric disorder among children and adolescents.1 Up to 12% of children in the United States2 and 6.5-7.6% of children in Korea were reported to have ADHD.3,4 According to the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV), the core symptoms of ADHD consist of inattention, hyperactivity, and impulsivity.5 In addition to the core symptoms, associated learning problems, social deficits, and psychiatric comorbidity are predictive of a worse prognosis.6,7
Norepinephrine (NE) has a crucial role in the attention control of the frontal cortex.8-10 Activation of the post synaptic α2 adrenergic receptor is related to the engagement of attention,9 and α2 adrenergic agonists have been shown to have beneficial effects on working memory and attention performance, and reduce distractibility. However, a higher level of adrenergic activation seems to have a detrimental effect on attention performance via α1 adrenergic receptor activation.10 Since the α1 adrenergic receptor has a lower affinity for NE than the α2 adrenergic receptor, higher levels of NE are required to activate the α1 adrenergic receptor. However, increased levels of NE induced by stress impair attention control mediated by prefrontal cortical function.10-12
α2 adrenergic agonists have been used to control the symptoms of ADHD.9,13,14 In ADHD, adrenergic activation is also related to increased attention performance via α2 activation.8 Excessive adrenergic activation has been suggested to lead to α1 activation and impaired attention performance.9 However, few studies have directly examined the relationship between α1 activation and attention impairment. Increases of cortisol are associated with the stress-induced NE release and α1 adrenergic receptor activation.15,16 Moreover, increase of cortisol level after stress is mediated by the activation of the adrenergic system and α1 adrenergic receptors.15 Increased NE during stress activates α1 adrenergic receptors of the corticotrophin- releasing hormone (CRH) containing cells in the paraventricular nucleus of the hypothalamus, which leads to an increased cortisol level.17
Activation of α1 adrenergic receptor mediates both cortisol level increase and attention impairment. Based on these findings, we speculated that cortisol increase during mentally challenging tasks is related to poor attention performance. Therefore, we undertook this study to examine whether increased cortisol level after a mentally challenging task is associated with poor attentional performance in ADHD youth. Since the increased variability in response time is one of the most consistent findings in the neuropsychological research of children with ADHD,18-22 we focused our study on the response variability of attention performance.
MATERIALS AND METHODS
Patients
Ninety clinic-referred children with ADHD participated in the study. A detailed protocol was described elsewhere, and data from a subsample were analyzed and published to address the relationship between stress reactivity and intellectual functioning.23 The participants were 6-15 years old and were mainly from the urban area of Seoul, Korea. ADHD was diagnosed using the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL). We excluded children with comorbid psychiatric disorder, medical illness requiring medication, or with a prior history of taking ADHD medication. Written informed consent was obtained from the parents of the children after the purpose and process of the study were explained. The protocol of this study was approved by the Institutional Review Board (IRB) at Kangbuk Samsung Hospital.
Psychological challenges
In previous studies, psychological testing, Trier Social Stress Test, or routine dental examination were used as stressors to evaluate the hypothalamo-pituitary-adrenal (HPA) axis reactivity in ADHD patients.24-28 Psychological testing was used as a stressor to activate the HPA axis reactivity. In the present study, we adopted a psychological test including the Korean-Wechsler Intelligence Scale for Children-Third Edition (K-WISC-III) and ADHD Diagnostic System (ADS).29 The Korean version of Wechsler Intelligence Scale for Children-III (K-WISC-III)30 was standardized among Korean children and adolescents. The WISC-III was developed to assess intellectual functioning in children 6-16 years of age, and consists of 13 individual subsets, including 10 standard and 3 supplementary subsets. The verbal intelligence quotient (IQ) test consists of subsets pertaining to information, similarities, arithmetic, vocabulary, comprehension, and digit span, while performance IQ consists of subsets pertaining to picture completion, coding, picture arrangement, block design, object assembly, symbol search, and mazes. The test takes 50-70 minutes to finish all 10 standard subsets. The ADHD diagnostic system (ADS)29 is a computerized continuous performance test that consists of auditory and visual modalities. In each modality, the target and non-target are presented in the form of auditory or visual stimuli. The test can be used to assess children over five years of age and consists of three sessions: early, middle, and late. The variables include omission error, commission error, response time, and variability in response time, which reflects the standard deviation of response time.
Cortisol determination in the saliva
All of the pre-test saliva samples were collected between 10 : 30 and 11 : 00 a.m. Participants were asked to take 30 minutes of rest before taking test. The patient's mouth was rinsed with water, and a saliva sample was taken 15 minutes before the WISC-III and ADS tests were performed. Thirty minutes after psychological testing, the patient's mouth was rinsed with water and a post-test saliva sample was collected.
The specimen was frozen at -20℃ to precipitate the mucin. The salivary cortisol concentration was determined by a standardized radioimmunoassay using the Diagnostic Product Corporation's Coat-A-Count Cortisol Kit (Los Angeles, CA, USA).
Evaluation of symptoms
In order to evaluate the severity of ADHD symptoms, the Abbreviated Conners Rating scale (ACRS)31 was used. ACRS is a standardized measure of ADHD symptoms which is frequently used to evaluate response to treatment progress in ADHD youth.32 The Korean version of the ACRS has shown adequate reliability.31
Dimensional measures of behavioral problems were obtained with the Korean-Child and Adolescent Behavior Checklist (K-CBCL).33 The K-CBCL consists of 114 items, each rated on a three tier scale: 0 (never), 1 (sometimes), 2 (frequently/severe). The scores of the CBCL were standardized among Korean children and adolescents.
The State-Trait Anxiety Inventory for Children (STAIC)34 was used to evaluate anxiety severity. The state anxiety score reflects the current level of anxiety, and the trait anxiety score reflects severity of trait anxiety in the past 2 weeks. A Korean version of the STAIC was developed, and showed good reliability and validity among Korean children and adolescents.
Parents were asked to complete the rating scales within a week prior to the psychological testing.
Statistical analyses
The patients with ADHD were divided into two groups, based on cortisol level change after psychological testing. Group 1 consisted of the patients who did not show any increase in cortisol level after the psychological testing, while group 2 consisted of the patients who showed an increase of cortisol level after testing.
To test whether the increase in cortisol level was related to the greater variability in response time, analysis of covariance (ANCOVA) was performed. The variability score for ADS was entered as a dependent variable, and the group was entered as a fixed factor. Interaction between anxiety and sustained attention ability has been reported.35,36 Since anxiety may influence the cortisol change after a task,37 we controlled the effect of anxiety.
Since response time variability is highly correlated with response time,21 we controlled the effect of response time. To control the effect of anxiety and response time on the variability in response time, these variables were entered as covariates. Statistical Package for the Social Sciences (SPSS) 13.0 (SPSS Inc., Chicago, IL, USA) was used and statistical significance was set at p < 0.05.
RESULTS
Sixty-eight out of ninety patients did not show an increase in cortisol level after psychological testing; these patients were designated as group 1. Children whose cortisol level increased were designated as group 2. Demographic data are presented in Table 1. There were no significant differences in age, gender, or scores of ACRS, CBCL, IQ test, and STAIC between group 1 and group 2 (Table 1).
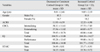
The ADS scores and cortisol levels are shown in Table 2. Group 2 revealed a significantly higher response time and response time variability values than group 1 (t = -2.655, df = 88, p = 0.009; t = -2.390, df = 88, p = 0.019, respectively).
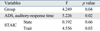
After controlling the effect of response time and anxiety, there was a significant difference in response time variability between the groups (Table 3).
DISCUSSION
The children whose cortisol level increased after psychological testing displayed more variability in response time than children and adolescents who showed no change or a decreased cortisol level. Perhaps, α1 adrenergic activation in both the paraventricular nucleus (PVN) and prefrontal cortex (PFC) would explain such a result. Hypothalamopituitary-adrenal (HPA) axis reactivity and PFC response to stress are closely related.16,17 NE activates α1 adrenergic receptors of the PVN, which releases CRH.16 PFC also has CRH receptors, and modulates the HPA axis reactivity to stress.17 Increased intra-individual variability in speeded-reaction-time (RT) tasks has a significant predictive power to differentiate between patients with ADHD and normal controls.22,38 Increased variability in response time is related to poor attention control by the frontal cortex.18,20 The result of the current study suggests that high levels of NE released by stress may induce poor attention performance in ADHD patients.
Although the mechanism is quite complex, it is likely that methylphenidate improves attention in part via α2 adrenergic receptor activation. However, overdose of methylphenidate may result in sympathomimetic symptoms, including agitation.39 On the other hand, stress-induced adrenergic over-activation can lead to distraction.40 Local infusion of alpha-1 adrenergic agonist (phenylephrine) into the prefrontal cortex impaired the spatial working memory performance in monkeys.41 Arnsten, et al.9 suggested that patients who show a high level of distractibility may receive a beneficial effect from α1 adrenergic blocking agents. Further research regarding the effect of α1 adrenergic blocking agents on attention performance is necessary.
In the present study, the test result of only the auditory modality of ADS was associated with increased cortisol level. This is highly likely because the auditory modality is more difficult than the visual one, thus likely being more sensitive to detect attention impairment.29
Age may26,42 or may not43 affect the cortisol level. We concluded that age distribution did not distort the result of this study, since there was no significant difference in age distribution between group 1 and group 2.
There was no difference in anxiety between groups 1 and 2. The result of the regression analysis also showed that increase of cortisol level was related to an increased variability in response time after controlling the effect of anxiety.
Several limitations may require cautions when interpreting the result of the current study. We found an association between increased cortisol levels after stress and greater response variability in an ADHD sample. Since we did not have a control group, it is not clear whether the obtained findings are specific to ADHD. HPA axis reactivity to Trier Social Stress Test for Children (TSST-C) was significantly higher in girls than boys,44 and HPA axis reactivity was greater for men than for women in provocative virtual environment.28 These findings suggest that HPA axis responses may be modified by the interaction of gender and stress protocols. Few studies have been performed on the relationship between gender and stress reactivity to ADS. In our data, there was no significant difference in gender distribution between group 1 and group 2. Small sample size might cause negative finding. In the future, gender effect on the stress response to ADS needs to be examined with larger sample size. HPA axis reactivity is responsible for activating the glucocorticoid response to stress.45 However, a discrete set of information from brainstem aminergic/peptidergic afferents, bloodstream, limbic circuits and prefrontal cortex is also involved in HPA axis reactivity.46 In this study, we inferred α1 adrenergic activation from cortisol increase. As we did not directly measure and isolate α1 activity, we could not exclude the possibility that other factors might have also influenced the result. The attention performance in the prefrontal cortex is also regulated by other transmitters than noradrenalin.40,47 We did not take other neurotransmitters into consideration in this study. Consequently, we might have oversimplified the result. ADHD is a heterogenous neurodevelopmental disorder.1,47,48 In this study, only some of the patients with ADHD showed negative impact of stress on performance. Differential response of ADHD subtypes to stress has been suggested.49,50 The present result is likely to apply only to subgroup of patients with ADHD. Future study could aim at resolving subtype impact of stress on performance with larger sample size.
In spite of these limitations, the result of the current study suggests that stress-induced cortisol increase may be associated with poor attention performance in ADHD patients. The clinical implication of this study is that stress may worsen the attention performance and learning abilities of children with ADHD. According to our finding, children with ADHD who demonstrate significant change in cortisol are likely to function better in a less stressful educational environment. Further longitudinal research is needed to examine the relationship between ADHD and anxiety which may be exacerbated by stress, and to evaluate the potential to mediate response through stress reduction techniques such as relaxation, exercise or cognitive behavioral therapy.

 XML Download
XML Download