

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The tolerability of infant vaccines has increased significantly since the introduction of modern acellular pertussis DTaP vaccines as replacements of more reactogenic whole-cell pertussis DTwP combination vaccines. This has led to increased acceptability by parents, improving coverage and compliance with recommended schedules. However, DTaP vaccines offer more than just better reactogenicity – they are the result of modern technology with better manufacturing consistency, and can be used as a platform on which to build combination vaccines containing the additional antigens recommended in schedules such as the Expanded Program on Immunization of World Health Organization (WHO) (1). These include inactivated poliovirus vaccines (IPV), an important element in the polio eradication strategy, Hepatitis B (HBV), and Haemophilus influenzae type b (Hib). Use of combination vaccines, by minimizing the number of injections required, offer simpler administration schedules and enhanced compliance, and allow for inclusion of new vaccine into routine schedules.
The Sanofi Pasteur diphtheria, tetanus, acellular pertussis (DTaP), HBV, IPV and Hib (PRP~T) antigens are well established, with a long history of effective use as separate vaccines or as components of DTaP–combination vaccines (2,3). In general, as a necessity for their approval for licensure, combination vaccines must elicit the same immunogenic responses as the individual components when given as separate injections or, if not, achieve levels that are considered clinically relevant. The decreased anti-Hib responses observed with some DTaP-Hib combinations when compared with DTaP and Hib given separately has been the subject of considerable debate (4). The clinical irrelevance of this decreased response is well established as countries where Hib vaccination is routine, and administered in the form of DTaP-Hib combinations with toddler boosters, have achieved the virtual eradication of Hib disease (5).
This decrease in Hib disease in countries with high vaccination compliance led to the WHO recommendation for the implementation of Hib vaccination in all countries (6). To facilitate the inclusion of Hib in those countries already routinely using DTaP vaccines, Sanofi Pasteur have developed various DTaP-Hib combinations, with or without other antigen components. One such combination is Pentaxim™, a DTaP-IPV//Hib combination, based on the components of the separate Tetraxim™ (DTaP-IPV) and Act-Hib™ (Hib) vaccines. The present study was performed in Korea, where Tetraxim™ and Act-Hib™ are the current standard of care, to demonstrate the non-inferiority of Pentaxim™ in this population as part of its licensure.
MATERIALS AND METHODS
Subjects
Intended subjects were Korean infants who were eligible for inclusion if they were 2 months-old (56–70 days) on the day of enrolment, had been born full-term (≥ 37 weeks) with at least 2.5 kg birth-weight, were able to attend all the scheduled study visits, and were healthy according to medical examination on the day of the first study visit.
Exclusion criteria included prior receipt of any of the study vaccine types (DTP, IPV or OPV, or Hib) or serologic evidence of infection with any of these diseases, any participation or intended participation in another clinical study, and any known medical conditions that could affect immune responses to vaccines. Such conditions included congenital immunodeficiency, immunosuppressive therapies, receipt of blood-derived products, or family history of immune disorders. Other chronic medical conditions leading to exclusion included known hypersensitivity to any of the vaccine components, and evidence of chronic infections such as Hepatitis B, Hepatitis C or HIV, thrombocytopenia or a bleeding disorder.
Study design
Following enrolment, at their first study visit infants were randomized to one of the two study groups using randomization envelopes supplied by the study sponsor. After a first blood draw infants in each group received their first vaccinations, either one dose of each of the current routine vaccines, DTaP-IPV and Hib (Group 1) or one dose of the combined DTaP-IPV//Hib vaccine (Group 2). Infants were monitored by the investigator or designated study personnel for 30 minutes for any immediate reaction. This procedure was then repeated at 4 months and 6 months of age. Infants returned for a final study visit at 7 months of age for a second blood draw and safety follow-up.
Study vaccines
All vaccines were manufactured and supplied by Sanofi Pasteur (Marcy L'Etoile, France). The licensed DTaP-IPV vaccine (Tetraxim™; lot E0278-1) contains ≥ 30 IU diphtheria toxoid, ≥ 40 IU tetanus toxoid, 25 µg pertussis toxoid (PT), 25 µg filamentous hemagglutinin (FHA), 40 units inactivated type 1 poliovirus D antigen, 8 units inactivated type 2 poliovirus D antigen, and 32 units inactivated type 3 poliovirus D antigen, with 0.3 mg Al(OH)3 in each 0.5 mL dose. The licensed Hib vaccine (Act-Hib™; lots D0901-1 and E0748) is supplied as a lyophilized powder containing 10 µg polyribosylribitol phosphate (PRP) chemically conjugated to 24 mg of tetanus toxoid (PRP~T) per dose that is reconstituted in 0.5 mL injectable saline for use. The combined DTaP-IPV//Hib vaccine (Pentaxim™; lot G2012-1) contains the same components as the DTaP-IPV and Hib vaccines, but the lyophilized Hib component is reconstituted in the liquid DTaP-IPV vaccine for use. Vaccines were administered by intramuscular injection in the anterolateral aspect of the upper thigh, DTaP-IPV and DTaP-IPV//Hib the right thigh, Hib vaccine when given separately in the left thigh.
Immunogenicity evaluation
Sera prepared from blood (5 mL) drawn before the first vaccination(s) at the first visit, and one month after the third, were stored at -20ºC to -80ºC for shipping to a laboratory qualified by Sanofi Pasteur Global Clinical Immunology for immunological assays. Anti-diphtheria antibodies were assessed by a neutralization test (SN) on Vero cells compared with the WHO equine antitoxin standard, and reported in IU/mL. Anti-tetanus antibodies were measured by ELISA calibrated against the WHO human standard TE3 and expressed in EU/mL. Anti-poliovirus antibodies to each of the three serotypes were assayed by a microneutralization test using the WHO standardized procedure (WHO/EPI/GEN 93.9) and expressed as the reciprocal of the highest dilution that inhibited the cytopathic effect of the challenge viruses (Mahoney, MEF-1, Saukett). Responses to pertussis antigens, PT and FHA were assayed by ELISA and expressed in EU/mL. Antibodies to the Hib vaccine component (PRP) were measured by RIA with the FDA human reference as standard, and expressed in µg/mL.
Safety evaluation
Parents were supplied with diary cards on which to record occurrence and measurements of solicited injection site (local) and systemic reactions, including daily axillary temperature, from Day 0 to Day 7 after each vaccination, and any unsolicited adverse event (AE) occurring from Day 0 to the next study visit. Adverse events considered related to the vaccination were termed adverse reactions (AR), solicited reactions occurring from Day 8 were considered unsolicited adverse reactions. Parents were reminded by telephone call on Days 3–5 to complete the diary card, and asked whether any reactions had occurred. Reactions were graded for severity by parents using pre-defined scales (Table 1).
Table 1
Definitions of severity grades for solicited local and systemic reactions

Serious adverse events (SAE) or adverse events necessitating medical assistance other than minor medical problems expected in an infant population, e.g. upper respiratory tract infections, were to be reported immediately to the study sponsor. The investigator assessed the causality of adverse events with vaccination at each subsequent study visit as either not related or related to the vaccination(s).
Statistical analysis
For immunogenicity assays the geometric mean concentrations (GMCs) or titers for poliovirus (GMTs) and the geometric mean titer ratios (GMTRs) comparing post-vaccination to pre-vaccination values were calculated with their 95% confidence intervals (CI) using the normal approximation (Student's t distribution with n-1 degree of freedom) after log10 transformation of the titers/concentrations. Seroprotection rates were calculated as percentages of each study group achieving accepted cut-offs indicative of seroprotection (≥ 0.01 IU/mL for diphtheria, ≥ 0.01 IU/mL for tetanus, ≥ 1:8 dilution for poliovirus, ≥ 0.15 μg/mL for PRP~T) with 95% CIs using the exact binomial method (Clopper-Pearson). For pertussis antigens, for which there is no serologic correlate, seroresponse rates were calculated as percentages of each group achieving at least a four-fold increase in antibody concentration from pre- to post-vaccination, with their 95% CIs using the exact binomial method.
For each antigen, non-inferiority was demonstrated if the 95% CI of the difference in seroprotection/seroresponse rates (combined vaccine minus separate vaccines), calculated based on the Wilson score method without continuity correction as described by Newcombe lay entirely above the clinically acceptable limit for non-inferiority (-d, with d set at 10%) (1-sided equivalence test, α = 2.5%) (7,8). The primary objective was reached if the non-inferiority was proven for each antigen, the conclusion being that the investigational vaccine was non-inferior to the control vaccines in terms of immunogenicity. Safety and reactogenicity data were analyzed descriptively.
Ethics statement
This was a phase III, multicenter, open, randomized, controlled clinical trial performed from September 2010 until March 2012. The protocol was registered on ClinicalTrials.gov (NCT01214889) and approved by the institutional review board of each study site. The study was performed according to the current Declaration of Helsinki, ICH and the Korean GCP at the time of the trial (27 June 2008). Parents or legal guardians were contacted by the study sites to obtain informed consent before enrolment into the trial. The primary objective was to demonstrate non-inferiority, in terms of seroprotection rates or vaccine response rates, of a three-dose primary series of DTaP-IPV//Hib (Pentaxim™) combined vaccine versus the separate DTaP-IPV (Tetraxim™) and Hib (Act-Hib™) vaccines currently licensed for use in Korea.
RESULTS
Subjects
Four of the 418 infants originally enrolled were excluded following unsuccessful venipuncture for the initial blood draw, leaving 414 who were randomized to the two study groups, 206 and 208 in the separate (DTaP-IPV and Hib) and combined (DTaP-IPV//Hib) groups, respectively. Demographics of the two study groups were similar (Table 2). Of those randomized 203 received at least one dose of both the DTaP-IPV and Hib vaccines, and 209 received at least one dose of the combined DTaP-IPV//Hib vaccine, two subjects in the separate group receiving the combined vaccine due to a randomization error and one being administered with an expired Hib vaccine (Fig. 1). There were 34 exclusions from the per protocol analyses due to protocol deviations (22 and 12 from the separate and combined vaccines groups, respectively). The most frequent protocol violation was not respecting the study schedule and reporting outside of time windows for vaccination or blood draws.

Immunogenicity
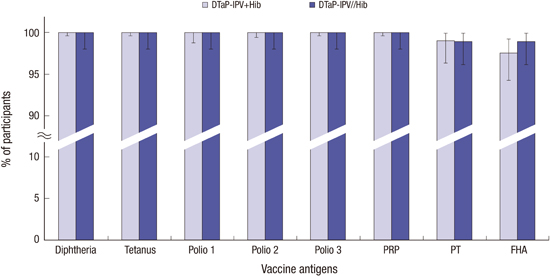
The primary objective, to demonstrate non-inferiority of the seroprotection/seroresponses to the antigens in the combined vaccines compared with separate administration, was met. The lower bounds of the 95% CIs of the difference between the separate groups minus the combined group were greater than -10% for all antigens, so non-inferiority was shown. Indeed, the robust immune responses to all antigens in both study groups were such that 100% of children achieved protective antibody cut-offs for diphtheria, tetanus, the three poliovirus serotypes, and PRP~T, and 99.0% had seroresponses to pertussis toxoid and 97.5%–99.0% to FHA (Fig. 2).
Fig. 2
Proportions of the two study groups achieving the respective protective antibody cut-offs, or a seroresponse for the pertussis antigens, at month 7 (with 95% CI).
CI, confidence interval; DTaP-IPV, diphtheria-tetanus-acellular pertussis-inactivated polio; PRP, polyribosyl ribitol phosphate; PT, pertussis toxin; FHA, filamentous hemagglutinin.

The GMCs/GMTs to the vaccine antigens one month after the third vaccinations were similar in both groups, with the exception of PRP~T (Table 3). There were robust immune responses to the diphtheria, tetanus, poliovirus and pertussis antigens, shown by the large GMTR for postvaccination to baseline antibody levels.
Table 3
Geometric mean concentrations (D, T, PRP, PT & FHA) or titers (polio) of antibodies to vaccine antigens in the two study groups (per Protocol) before and after the three dose vaccination series, and Geometric Mean Titer Ratios (GMTR) of Post- to Pre-vaccination values (with 95% CI)
The responses to PRP~T were also large, but the GMC in the combined group (11.0 µg/mL) was approximately half that observed in the separate DTaP and PRP~T group (23.9 µg/mL), a known effect when Hib vaccines are administered in combination with DTaP combination vaccines. However, the lower GMC was similar to those achieved by other vaccines in Korean infants (9), and 100% had protective titers (0.15 µg/mL). Further, 98.3% and 97.4% in separate and combined groups, respectively, had titers ≥ 1 µg/mL, a level indicative of long-term protection (10). The WHO definition of an effective Hib vaccine is 70% of infants achieving titers ≥ 1 µg/mL one month after completion of the vaccination series (6).
Reactogenicity
All vaccinations were generally well tolerated, the majority of reported reactions being Grade 1 or 2 in intensity and resolving with the 7 days postvaccination period. There were 30 SAEs reported, 12 in the separate group and 18 in the combination group, only one of which resulted in withdrawal of the infant from the study by the investigator (Table 4). The majority of these (23) were cases of typical infections (RSV bronchiolitis, pneumonia, etc.) expected within an infant population (6 and 17 in separate and combined groups, respectively). The SAE that resulted in withdrawal was a case of Kawasaki's disease in a girl in Group 1. Symptoms (fever and poor oral intake) were observed 19 days after her first pair of vaccinations with DTaP-IPV and Hib, and 8 days after receiving Prevenar® and Rotarix® vaccines, leading to hospitalization when symptoms aggravated 3 days later. Following treatment she fully recovered 14 weeks later. Although the event was considered to be unrelated to the vaccination she was withdrawn from the study.
Table 4
Safety and reactogenicity after any vaccination of the safety set
After any dose (pooled data), 75.6% of the subjects vaccinated with separate DTaP-IPV and Hib vaccines experienced at least one solicited injection site reaction and 86.6% at least one solicited systemic reaction (Table 4). In subjects who received the DTaP-IPV//Hib combination vaccine 75.6% experienced at least one solicited injection site reaction and 80.9% at least one solicited systemic reaction.
All solicited injection site reactions occurred within 3 days of vaccine administration, were of Grade 1 intensity, and the majority resolved within 8 days after any injections. In both groups, tenderness (58.2% and 53.2% at DTaP-IPV and Hib sites in Group 1, 61.2% at the DTaP-IPV//Hib site in Group 2) was the most frequently reported injection-site reaction. Erythema and induration occurred at similar rates at DTaP-IPV and DTaP-IPV//Hib sites, but were less frequent at the Hib site when administered separately.
Most solicited systemic reactions occurred within 3 days of vaccine administration and resolved within 7 days after any injections, and were of Grade 1 intensity, except for irritability, which was usually Grade 2. Overall, irritability (53.7% and 51.2% in Groups 1 and 2, respectively), drowsiness (50.7% and 49.3%, respectively), and abnormal crying (54.7% and 48.3%, respectively) were the most frequently reported solicited systemic reactions. Fever was the least frequent solicited systemic reaction in both groups, 11.4% and 15.9%, respectively, and no case of fever > 39.5°C was reported.
Although rates of erythema and swelling increased with subsequent doses, there were opposite trends for tenderness and for most systemic reaction rates to decline with subsequent doses (Fig. 3). The only exception was fever, which increased from 6.3% and 3.2% in separate and combined groups, respectively, after the first dose, to 7.0% and 7.3% after the third dose.
Fig. 3
Proportions of each study group (95% CI bars) reporting solicited local and systemic reactions in the two study groups after each dose. Local reactions are shown for each vaccination site (DTaP-IPV, Hib, and DTaP-IPV//Hib).

Unsolicited adverse events, and solicited reactions occurring after the 7 day postvaccination window, occurred at similar rates in both groups (Table 4). The majority of the unsolicited AEs were not serious and consisted mainly of typical infant infections. Most reactions reported after the 7 day period were cases of persisting injection site induration and nodules.
DISCUSSION
Combination infant vaccines based on a backbone of diphtheria, tetanus and acellular pertussis (DTaP) have been introduced into routine infant vaccination schedules over the last twenty years, initially in developed countries where they are now ubiquitous, and more recently into developing countries. Their introduction was a consequence of the perception of high reactogenicity with whole-cell pertussis (DTwP) vaccines (11), but they also offer other significant advantages over DTwP, most notably as in manufacturing; purified acellular antigens are easier to standardize than the whole cell preparations, which has previously been shown to been manufactured with variable potencies (12-14). The DTaP backbone has subsequently been expanded with the inclusion of additional infant antigens so that hexavalent vaccines, including hepatitis B, inactivated poliovirus and Hib antigens, are now the standard of care in many countries. Future combinations may include more antigens, e.g. meningococcal conjugates, which are currently administered concomitantly with the DTaP-combinations, but may be included on heptavalent combinations (15).
Inclusion of additional antigens into combination vaccines is dependent upon them being administered in the same schedule, all components being equally immunogenic when administered in the combination and not significantly affecting the tolerability of the overall combination. For this reason, new combinations are tested to ensure non-inferiority of the immune responses to the included antigens compared with separately administered vaccines. The Hib (Act-HIB™) vaccine used in the present study, which is the current standard of care in Korea, was licensed following demonstration of its safety and immunogenicity in Korean children (16). Similarly, the DTaP-IPV (Tetraxim™) combination was shown to be safe and highly immunogenic for all antigens when given at 2, 4, and 6 months of age in Korean infants, and non-inferior to the responses to separate DTaP and IPV components (17). In the present study, we have shown that the immune responses to DTaP-IPV//Hib combined vaccine (Pentaxim™) were non-inferior for all vaccine antigens to the separate vaccines according to the predefined criteria used in the study.
A concern with the introduction of DTaP//Hib combinations was the potential clinical consequence of a lower response to the Hib component than when given as a separate vaccine (3). Not observed with all DTaP//Hib combinations, and most evident after the infant primary series of vaccinations, there did not appear to be any clinical consequences; introduction of DTaP//Hib combinations was accompanied by the virtual eradication of Hib infections in developing countries (5,18,19). In this study there was also a significant decrease in response to Hib when administered in combination with the DTaP (11.0 µg/mL) compared with separate injection (23.9 µg/mL). However, the very high concentrations achieved by both separate and combined administration, with > 99% having concentrations considered protective (0.15 µg/mL), and 97.4% of the combined vaccine group having a level (≥ 1.0 µg/mL) indicative of long-term protection (10) suggest this is not an issue. The GMC achieved with DTaP//Hib is higher than those reported with the combinations routinely used in Europe and the USA that include PRP~T (3), and is similar to levels previously reported in Korean infants (9). Kim et al. (20) reported that 87.5%–98.4% of Korean infants achieved anti-PRP titers ≥ 1.0 µg/mL one month after a third dose of various PRP~T conjugates. Therefore it is unlikely that the difference in PRP antibody levels will have any clinical significance, especially as a booster dose of Hib vaccine is administered at 12–15 months of age in the Korean schedule.
All vaccines were well tolerated, the combined vaccine having a similar safety profile to the separate DTaP-IPV and Hib vaccines when given concomitantly in the same 2, 4, and 6 months schedule. Most solicited reactions were grade 1 or 2 in severity and transient, and resolved within 3 days of vaccination. Similar proportions of infants in both study groups had a solicited local reactions, but the use of two injections meant children in the separate DTaP-IPV and Hib groups had more local reactions overall. Systemic reaction rates were similar in both groups, and mainly grade 1 or 2 in severity. Importantly, no child in either group had grade 3 fever (> 39.5ºC).
Concomitant administration of multiple vaccines has been demonstrated to be safe and immunologically effective, but parents' desire to limit the number of injections required at one well-care clinic visit, and healthcare providers perception of this (21,22) may limit the number of vaccines that can be administered. Giving one less injection by using a combination vaccine decreases such concerns, as well as opening up the possibility of including another vaccine at each visit to allow for addition of new vaccines into the infant schedule. The present study demonstrates that the use of the combination DTaP-IPV//Hib vaccine, Pentaxim®, is immunologically non-inferior to the DTaP-IPV (Tetraxim®), and Hib (Act-Hib®), vaccines administered separately, the current standard of care in Korea. Use of Pentaxim® may improve compliance and allow for the introduction of new vaccines into the Korean infant schedule.
 XML Download
XML Download