

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Loss of scalp hair is not a serious life threatening disorder, but it can cause psychological distress and affect quality of life adversely. Hairs are rapidly proliferating organ with much requirement of blood supply. Therefore, the relationship between micronutrients and hair loss has been evaluated in several studies since the 1960s (1). The most widely cited nutritional causes of hair loss include iron, one of the key micronutrients in metabolism of our body. From its diverse functions, it is well known that iron deficiency (ID) is associated with a lot of pathological conditions (2). However, its role in hair loss is not well established yet.
When reviewing articles which have documented the relationship between ID and hair lossincluding female pattern hair loss (FPHL), telogen effluvium, alopecia areata, alopecia universalis or totalis, some (3-7) advocated the association between ID and hair loss and others were against it (8-12). This controversy might be caused by study designs, methodology and clinical condition defining hair loss.
For detection of ID, serum ferritin level can be used as a very early marker. It is a main iron-binding protein in nonerythroid cells reflecting total body iron stores. It decreases from very early stage of ID as iron reserves go down (2). Because only ID can cause very low serum ferritin concentration (FC), a FC is very specific for ID (13). However, it can play a role in inflammation as a reactive protein, patients with active infection and/or inflammation should not be included in the analysis when we consider FC is used for detecting ID. Hormonal status can affect hair loss and it should be considered when interpreting the clinical condition, too.
This study was designed to find out evidence about association between ID and hair loss. Current studies only concerned of females, but not male subjects. Although females have more issues about ID in general, hair loss is common problem in males, too. Therefore, we also analyzed the effect of ID among patients with male pattern hair loss (MPHL).
MATERIALS AND METHODS
Retrospective chart review on patients with hair loss was conducted. Medical data for patients who had visited our hair clinic from January 2010 to February 2011 and been diagnosed as FPHL or MPHL were obtained. Among them, patients who had more than 6 months of history of hair loss and had not received any kind of treatments for their hair loss were enrolled in the analysis. Patients who had visited for their regular check-up of general health condition and did not suffer from hair loss were selected for a normal control. They were matched by age and sex with hair loss patients. The database includes diagnosis, physical examination findings, laboratory data, medication lists and medical history. FPHL was diagnosed as central scalp hair loss with or without frontal accentuation with hair miniaturization and no signs of scarring alopecia (14). MPHL was defined as non-scarring progressive miniaturization of the hair follicle with a usually characteristic pattern distribution in genetically predisposed men (15). MPHL patient was classified according to basic and specific (BASP) scale for further analysis (16).
All patients in the analysis underwent biochemical investigation at the first visit. It included thyroid function tests, complete blood count with erythrocyte sedimentation rate (ESR), renal and liver function tests, and iron studies (FC, iron, total iron binding capacity [TIBC] and hemoglobin). Follow up FC and complete blood cell count with ESR was checked on patients who had received iron supplementation. All of these tests were performed at our institution using the same laboratory system. The biochemical investigation in age/sex matched normal control patients were analyzed, too.
Patients or their controls who had evidence of active infection or inflammation and who were or had been pregnant within previous 12 months were excluded because those factors can influence FC. Those who had abnormal thyroid function results were also excluded from the analysis. Those currently taking iron supplements due to other cause were also excluded.
To assess the clinical outcome of iron supplementation, Patient Global Assessment (PGA) and Patient Satisfaction (PS) score were recorded several months (at least 6 months) after the supplementation. PGA was graded into 5 categories, as worse, unchanged, slightly improved, moderately improved and much improved. PS was graded into 4 classes as unsatisfied, slightly satisfied, satisfied and very satisfied.
Subgroup analysis
Female patients with hair loss were divided into two subgroups according to their menstrual status. Male patients with MPHL were classified into M dominant, and F dominant type using BASP scale to see difference between two types (16).
Statistics
Basic frequencies and prevalence rates were calculated for demographic data and other parameters. The χ2 test or Fisher's exact test was performed to compare observed frequencies. P values less than 0.05 were considered as a statistical significance. To compare patients with normal healthy controls, Student t-test was conducted. Regression analysis was done to see relation between age and other parameters.
RESULTS
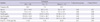
There were 210 patients diagnosed as FPHL (113 women) or MPHL (97 men) who met the inclusion criteria of this study. Age-sex matched healthy 210 controls (113 women and 97 men) were compared. Age of enrolled patients was 42.9 ± 13.0, and 32.5 ± 9.6 yr old for FPHL and MPHL group respectively, showing later onset of FPHL (P < 0.001) (Table 1). Hemoglobin levels were normal in all groups. FC was 49.27 ± 55.8 and 77.89 ± 48.32 µg/L in FPHL patients and its age/sex-matched controls respectively. MPHL patients showed 132.3 ± 72.1 µg/L of FC, while 210.92 ± 53.22 µg/L of FC was observed in its age/sex-matched controls. Iron concentration was 90.89 ± 43.50 µg/dL and 88.49 ± 38.23 µg/dL for FPHL and its controls. Patients with MPHL showed 115.13 ± 40.94 µg/dL of iron concentration while healthy men without hair loss showed 122.33 ± 59.84 µg/dL. TIBC was 346.30 ± 57.4 µg/dL and 319.85 ± 49.6 µg/dL for FPHL and MPHL, respectively (Table 1).
FPHL group was classified according to menstrual state. FC in patients with FPHL before menopause was 30.67 µg/L on the average while patients after menopause showed mean FC of 83.22 µg/L (P < 0.001).For healthy controls before menopause, higher FC level was detected (69.32 ± 33.92 µg/L). However, postmenopausal healthy control showed almost same FC compared with patients with hair loss (83.22 ± 76.92 µg/L vs 85.38 ± 21.22 µg/L) (Table 2).
MPHL group was subdivided into M or F type by BASP classification. There were 58 M type, 7 F type and 31 miscellaneous patients. Mean hemoglobin, FC, iron, TIBC was 15.3 ± 1.0 g/dL, 133.55 ± 60 µg/L, 120.58 ± 53.9, 315.27 ± 50.8 µg/dL for M type patients and 15.3 ± 1.6 g/dL, 123.00 ± 63.8 µg/L, 112.60 ± 48.7, 314.50 ± 43.0 µg/dL respectively for F type patients. F type showed slight lower values compared to M group. However we did not find any significant differences among three groups. Patients with FC < 70 µg/L were more frequently noticed in M group (17.2%) than F group (7.35%),which was not statistically different. There was no correlation between onset age and FC in MPHL patient (r = 0.12) (Table 3).
Patient whose FC was less than 70 µg/L, had been put on oral iron supplementation for several months. PGA of iron supplementation group and other treatment group was not much different (P = 0.10). PS of iron supplement group was 2.11, which was lower than that of non-supplement group (2.23) but not statistically significant (P = 0.29). PGA was 3.05 vs 2.91 (P = 0.46) in iron supplementation group of FPHL vs non supplementation group of FPHL which was slightly higher in supplementation group but not significantly different. However, patients with MPHL rated lower PGA and PS when they had been on oral iron supplementation (Table 4).
Patients who had received oral iron supplementation had follow-up laboratory test for FC and hemoglobin. In general, FC doubled after 6 months of supplementation (325 mg of ferrous sulfate twice a day: elemental iron content 65 mg) (35.8 ± 25.5 µg/L to 62.5 ± 37.9 µg/L) (P < 0.001) but hemoglobin level did not alter after iron supplementation. (13.1 ± 1.5 to 13.1 ± 1.8 g/dL, P = 0.5).
DISCUSSION
The association between ID and hair loss is still a debating issue. Kantor et al. (5) reported that alopecia areata, FPHL and telogen effluvium patients under 40 yr old showed lower serum ferritin concentration than controls without hair loss. Rushton et al. (7) also demonstrated that there was significant decrease of hair loss and increase of FC in patients with telogen effluvium who received oral iron therapy. These results are supported by Moeinvaziri et al. (3) who suggested that serum FC and transferrin saturation is lower in patients with telogen effluvium based on the case control study design. In contrast, Sinclair (12) reported that response rates to iron supplementation were not different between low ferritin (< 20 ng/mL) and normal group (≥ 20 ng/mL) in FPHL patients. Olsen et al. (8) also showed no differences in prevalence of ID between female patients with (285 FPHL patients and 96 telogen effluvium patients) or without hair loss (a total of 76 Caucasian women older than 18 yr old). Rushton et al. (17) criticized study of Olsen et al. (8) in that it appears to have some confounding issues and contradictions such as no-standardized evaluation in blood sampling and no quantitative hair evaluation in control group.
Reviewing previous studies (3-6, 8-12), the role of iron in hair loss appears untangled until now. Therefore, we conducted this study in order to find out the relationship between body iron status and various conditions with hair loss. In order to overcome the limitation of retrospective study, we carefully selected patients diagnosed with FPHL and MPHL who had visited our clinic between January 2010 and February 2011 and underwent the screening test at their first visit. We excluded patients with abnormal thyroid function or any medical history which can affect body iron status (18). For the better comparison, age-sex matched healthy controls without complaint of hair loss were selected who had visited the hospital for a check-up which includes all blood tests of initial screening test.
ID is a continuum of various status of iron deposition in the body. Iron depletion is the mildest form of ID followed by iron-deficient erythropoiesis andiron deficient anemia being the most severe form (2). Body iron stores can be assessed by serum FC (13) but there is no consensus which ferritin level is the right one to define ID in practice. Although many laboratories use FC of 10 to 15 µg/L as the lower limits of normal based on reference sample groups, this only gives a sensitivity of 59% and a specificity of 99% for diagnosing iron deficiency (19). In women of childbearing age, using a cutoff of 10 to 15 µg/L yields a sensitivity of 75% and specificity of 98% in diagnosis of ID (2). A cutoff of 30 µg/L yields a sensitivity of 92% and a specificity of 98%, while a cutoff of 41 µg/L yields a sensitivity of 98% and a specificity of 98%. It might have contributed to the controversy that there is no guideline to define ID. From this study, over 80% of FPHL showed serum FC lower than 70 µg/L, while only less than 20% of age matched healthy female controls showed it. No female healthy controls showed serum FC lower than 30 µg/L in this study. Therefore, serum FC lower than 30 µg/L might be a clinically significant indicator for ID especially in female hair loss patients considering their menstrual status.
In this study, patients with MPHL show relatively early onset age, which means they appear to visit the clinic earlier than those with FPHL. Patients with FPHL show definitely lower serum FC compared with age/sex-matched normal controls. Female patients with FPHL were divided into two groups based on their menstrual status. Premenopausal patients with FPHL demonstrate much lower serum FC than postmenopausal FPHL patients. When compared with normal age/sex matched controls, statistically significant low serum FC is observed in FPHL premenopausal patients, while it is not significantly different between FPHL patients and normal controls after menopause. This result implicates that ID plays a certain role in premenopausal female patients with FPHL. However, weak association of ID with FPHL in postmenopausal patients could be addressed from this study.
Patients with MPHL show considerably lower serum FC on the average than age-sex matched healthy controls, although the serum level of FC is within normal range. We failed to prove the correlation between onset age and serum FC in MPHL patient, either (r = 0.12). However, approximately 20% of MPHL show serum FC lower than 70 µg/L and their age matched controls do not show that low serum FC. This result implicates that screening of iron status in even male patients with hair loss might provide clinical benefits.
Clinical manifestations of F type of MPHL looks like those of FPHL in female patients (16). Therefore, we looked into patients with MPHL according to types (M type, F type and others based on BASP classification), which turns out there was no strong relationship between subtype of MPHL and ID.
Patients showing low FC level < 70 µg/L had been on oral ferrous sulfate (130 mg of elemental iron/day) and serum level of FC doubled after 6 months of supplementation. Clinical response to iron supplementation proves not to be much higher than expected. Especially patients with MPHL patients rated lower PGA and PS when they were on oral iron supplementation. Oral 5 alpha reductase inhibitor is the first line treatment to MPHL patients (20) and if MPHL patients showed lower FC, iron supplementation was first given to patients during almost 6 months until FC became higher than 70 µg/L. Therefore, iron supplementation group did not receive any kind of oral 5 alpha reductase inhibitor, which might cause significantly lower PGA and PS.
This study owns its value because it demonstrates the first direct comparison between hair loss patients and same number of healthy controls matched by age and sex. It strongly supports the previous studies that ID can be a certain factor of developing or worsening FPHL especially in premenopausal female patients. Its role in MPHL is hard to conclude from this study. However, screening for ID as the first evaluation of hair loss in even male patients might be worthwhile in the clinical field.



 XML Download
XML Download