

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hereditary breast and ovarian cancer syndrome (HBOC) is characterized by increased susceptibility to the development of breast, ovarian, and other cancers [1]. The significance of the BRCA1 and BRCA2 (BRCA1/2) germline variants as predictors of HBOC has been well established [2]. Identification of germline variants in BRCA1/2 has improved the prevention and diagnosis of HBOC [3]. However, BRCA1/2 pathogenic variants have been observed in only approximately 20% of suspected hereditary cases [4]; several other cases are suspected to be caused by germline pathogenic variants in other cancer-related genes [5].
Recent advances in genetic testing have led to the discovery of many genes that increase the susceptibility to cancer [5]. Furthermore, the development of next-generation sequencing (NGS) has enabled simultaneous testing of multiple genes. Many recent studies have examined the clinical validity of comprehensive multi-gene panel testing in breast and ovarian cancers [678]. It has been reported that 3% to 4% of high-risk patients have pathogenic variants in cancer-related genes other than BRCA1/2, but the exact prevalence details remain unknown [910]. Therefore, clear clinical management guidelines should be established, and evidence-based clinical validity of multi-gene panel testing should be conducted. In this study, we evaluated the clinical validity of multi-gene panel, including BRCA1/2 and 25 other cancer-related genes as a screening tool for patients with HBOC.
METHODS
Study population
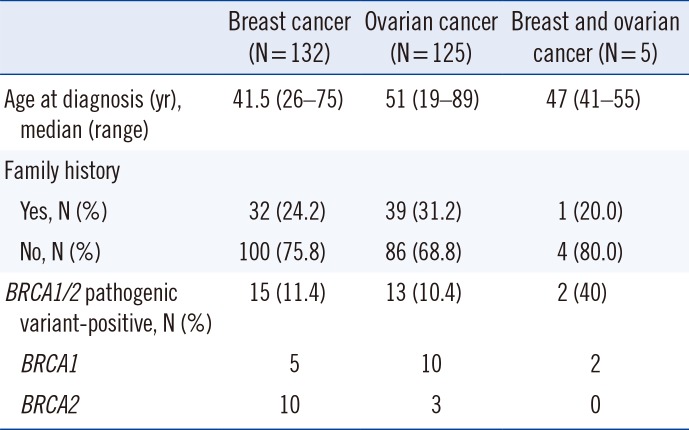
This was a retrospective study based on chart review and test results. We reviewed 262 patients with breast or ovarian cancer who underwent BRCA1/2 gene testing from May 2015 to July 2017 in Seoul St. Mary's Hospital, Seoul, Korea and met the National Comprehensive Cancer Network (NCCN) criteria for HBOC [11]. For inclusion, HBOC should be suspected in individuals with a personal or family history of any of the followings: (a) breast cancer diagnosed at or before the age of 45 years; (b) ovarian cancer; (c) multiple primary breast cancers either in one or both breasts; (d) triple-negative (estrogen receptor-negative, progesterone receptor-negative, and human epidermal growth factor receptor 2 [HER2/neu]-negative) breast cancer, particularly when diagnosed before the age of 60 years; (e) two or more relatives with breast cancer, with at least one under the age of 50 years; (f) three or more relatives with breast cancer at any age; and (g) a previously identified BRCA1 or BRCA2 pathogenic variant in the family. Medical and family histories were provided by the referring physicians and/or were collected through a review of the patients' medical records (Table 1).
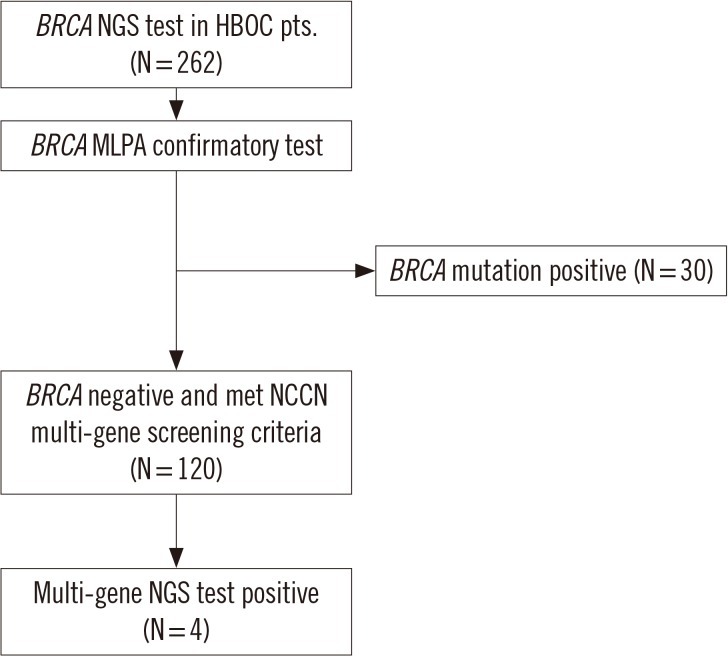
The BRCA1/2 test results of the 262 patients were evaluated. According to the BRCA testing strategy of our institution, patients who tested negative in the BRCA1/2 test but met the NCCN multi-gene testing criteria underwent cancer-related multi-gene panel testing (Fig. 1). The NCCN multi-gene testing criteria were as follows: (a) at least one case of breast or ovarian cancer in a first- or second-degree relative; (b) bilateral breast cancer; (c) a first diagnosis of breast cancer before the age of 40 years; and (d) co-diagnosis of breast and ovarian cancers in the same patient. In total, 120 HBOC patients were selected for the NGS multi-gene panel testing targeting cancer-related genes other than BRCA1/2.
Multi-gene panel testing was performed for 120 of the 232 BRCA1/2-negative patients, including 72 breast cancer patients, 47 ovarian cancer patients, and one patient with both breast and ovarian cancers. All patients previously provided informed consent for all tests, including the BRCA1/2 gene and multi-gene panel testing. This study was approved by the Institutional Review Board/Ethics Committee of Seoul St. Mary's Hospital, Seoul, Korea (KC15RISI0915).
Sample collection and preparation
Peripheral blood samples were collected from HBOC patients. Genomic DNA was extracted from whole blood using the QIAamp DNA Blood Mini Kit (Qiagen, Venlo, The Netherlands). Each DNA sample was checked for purity using a NanoDrop 1000 system (Thermo Fisher Scientific, Rockford, IL, USA), and DNA concentration was determined using a Qubit 3.0 fluorometer (Thermo Fisher Scientific). Extracted DNA was stored at −80℃ until further use.
BRCA1/2 variant testing using NGS
The library was prepared using the Ion Chef System (Thermo Fisher Scientific) according to the manufacturer's instructions. Briefly, barcoded libraries were generated from 10 ng of DNA per sample using the Ion AmpliSeq Chef Solutions DL8 Kit (Thermo Fisher Scientific) and the Oncomine BRCA Research Assay (Thermo Fisher Scientific). Two premixed pools of 265 primer pairs were used to generate the sequencing libraries. Clonal amplification of the libraries was performed by emulsion PCR using an Ion AmpliSeq IC 200 Kit (Thermo Fisher Scientific). Next, the prepared libraries were sequenced on an Ion S5 XL Sequencer using an Ion 520 Chip and an Ion 520 kit–Chef Kit (Thermo Fisher Scientific). Raw sequence data in FASTQ format were aligned to the hg19 human reference genome using the Torrent Mapping Alignment Program aligner implemented in v5.2 of the Torrent Suite software (Thermo Fisher Scientific). We used the plug-in Torrent Variant Caller v5.2.0.34 (Thermo Fisher Scientific) for single nucleotide variant (SNV) calling to generate a variant call format file. For Torrent Variant Caller analysis, the default settings of the germline low-stringency parameters (minimal variant frequency, 0.1; minimum variant quality, 10; minimum coverage, 5×; maximum strand bias, 0.98; and minimum variant score, 10) were used and candidate variants were obtained only at a variant frequency at a given position ≥20% and variant coverage ≥20×. Copy number variation (CNV) and insertions and deletions (indels) were evaluated using a single integrated workflow with the Ion PGM platform (Thermo Fisher Scientific, San Jose, CA, USA).
Multiplex ligation-dependent probe amplification analysis (MLPA) for CNV
Following BRCA1/2 NGS analysis, MLPA was conducted for BRCA1/2 (MRC-Holland, Amsterdam, The Netherlands) to identify or confirm any large genomic rearrangements (LGR). The inclusion criteria were: (a) early-onset breast cancer (diagnosed at ≤36 years); (b) two breast primaries (include bilateral disease or two or more ipsilateral primary tumors); (c) breast cancer diagnosed at any age, with ≥one close blood relatives (including first-, second-, or third-degree) with breast and/or epithelial ovarian cancer; (d) both breast and epithelial ovarian cancers diagnosed at any age; and (e) epithelial ovarian cancer with ≥one close blood relatives with breast and/or epithelial ovarian cancer, according to our previous study [12]. The MLPA results were analyzed using GeneMarker software (Softgenetics, State College, PA, USA). Peak heights were normalized, and deletions or duplications were defined as recommended by the manufacturer. Direct sequencing of the probe binding and ligation sites was performed for the relevant exons to detect nearby variants, which can lead to a false decrease in peak signal.
Multi-gene panel testing using NGS
Following BRCA1/2 variant testing, we conducted a multi-gene panel testing using NGS with a targeted capture sequencing panel (BRCA Reflex, Hereditary Cancer Research Panel, Thermo Fisher Scientific Inc., Waltham, MA, USA) that included all coding sequences and intron-exon boundaries of the coding exon from 25 hereditary cancer-related genes with a central role in DNA repair or the mismatch repair (MMR) pathway (APC, ATM, BARD1, BMPR1A, BRIP1, CDH1, CDK4, CDKN2A, CHEK2, EPCAM, MLH1, MRE11A, MSH2, MSH6, MUTYH, NBN, PALB2, PMS2, PTEN, RAD50, RAD51C, RAD51D, SMAD4, STK11, and TP53) [13]. NGS analysis was subsequently performed using the Ion Torrent S5 system (Life Technologies, Foster City, CA, USA). High-quality sequencing data with an average depth of 500–1,000-folds were acquired. Annotation of SNVs, indels, and splice-site alterations was performed using the Ion Reporter Server System (Life Technologies).
Confirmatory sanger sequencing
The detected pathogenic and likely pathogenic variants identified by NGS analysis were verified by Sanger sequencing. Direct sequencing of entire coding exons and flanking intronic sequences of relevant genes was performed bi-directionally on an ABI 3130XL Genetic Analyzer (Applied Biosystems, Foster City, CA, USA) with a BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems). Chromatograms were analyzed with Sequencher software version 5.0 (Gene Codes, Ann Arbor, MI, USA). Sanger sequencing was performed as described previously [14]. Exon numbering and DNA sequence variant descriptions are based on NM_007294.3 and NM_000059.3 as reference sequences for BRCA1/2. The reference sequences for CHEK2, MLH1, MSH2, PALB2, and PMS2 are as follows: CHEK2 NM_001005735.1, MLH1 NM_000249.3, MSH2 NM_000251.2, PALB2 NM_024675.3, and PMS2 NM_000535.6.
Genetic variant classification
Genetic variants were classified using a five-tier system according to the guidelines of the American College of Medical Genetics and Genomics (ACMG): pathogenic, likely pathogenic, variant of unknown significance (VUS), likely benign, or benign [15]. Pathogenic and likely pathogenic variants were considered significant.
Statistical analysis
Normally distributed continuous variables were summarized as mean±SD and compared using the Student t-test. Patient age was summarized as median (range). All tests were two-tailed. P≤0.05 was considered statistically significant. Statistical analyses were performed using MedCalc version 15.5 (MedCalc, Ostend, Belgium).
RESULTS
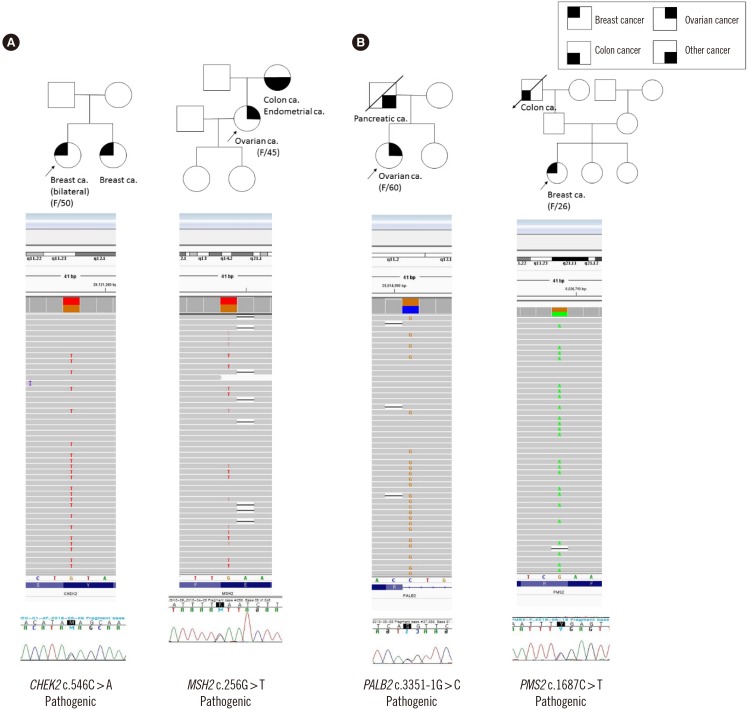
Pathogenic or likely pathogenic variants in BRCA1/2 were detected in 30 patients (30/262, 11.5%). Of the patients included in the multi-gene panel testing group, 3.3% (4/120) carried a pathogenic variant: two ovarian cancer patients and two breast cancer patients. The median age at diagnosis was 46.5 years (range 26–60 years) (Fig. 2). All four patients had a family history of cancer. The variants identified were MSH2 (c.256G>T, p.Glu86*, pathogenic), PMS2 (c.1687C>T, p.Arg563*, rs587-778618, pathogenic), CHEK2 (c.546C>A, p.Tyr182*, rs2009-17541, pathogenic), and PALB2 (c.3351-1G>C, pathogenic). The variants in MSH2 and PALB2 have not been previously identified. These variants cause premature termination or a splicing error and are classified as pathogenic or likely pathogenic, according to the ACMG criteria (Evidence PVS1, PM1, PM2, PP3-5) [15]. Additionally, a missense variant in the MLH1 gene (c.1937A>G p.Tyr646Cys, rs35045067) of a breast cancer patient was classified as VUS.
Patients with a variant in BRCA1/2 or cancer-related genes (N=34) had a family history of cancer in a second-degree or closer relative more often than those without a detected variant (40.0% vs 28.4%, P=0.023). In one patient with PMS2 variant, the breast cancer recurred one year after surgery and completion of chemotherapy.
DISCUSSION
We performed a multi-gene panel test using NGS analysis and evaluated its clinical validity in HBOC patients, focusing on patients negative for pathogenic variants in the BRCA1/2 NGS testing.
BRCA1/2 pathogenic variants were detected in 11.5% of HBOC patients. This result is lower than that reported by the Korean Hereditary Breast Cancer (KOHBRA) large-cohort study (15.73%, 378/2,403) [16]. The difference could be due to the different characteristics of the two studies. The KOHBRA study was a prospective study targeting only breast cancer patients; trained research nurses visited the institution and obtained disease history up to at least three generations back, including third-degree relatives [16]. In contrast, our study targeted breast and ovarian cancer patients and was a retrospective study based on chart review and test results. The advantage of our study is that it reflects real-life clinical situations.
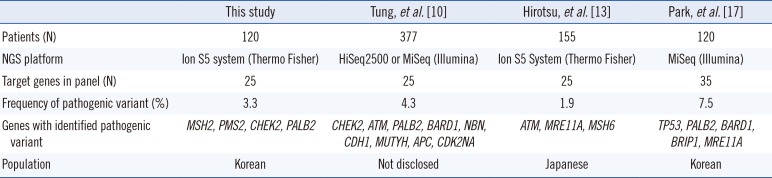
The frequency of pathogenic variants in 25 hereditary cancer-related genes in our study is in line with previous findings (Table 2) [101317]. All these studies selected BRCA1/2-negative breast and/or ovarian cancer patients. Tung, et al. [10] reported that 2.9% of the 377 patients had pathogenic variants in breast/ovarian-associated genes but were negative for BRCA1/2 variants. Hirotsu, et al. [13] observed that 1.9% (3/155) of patients possessed a pathogenic variant in genes that have a central role in DNA repair or the MMR pathway.
The pathogenic variants identified in MSH2, PMS2, and CHEK2 are nonsense variants. MSH2 is an MMR gene, and pathogenic variants in it can lead to Lynch syndrome or hereditary nonpolyposis colorectal cancer syndrome. Nonsense variants, are the most common cause of MMR function deficiency, comprising 82% of MSH2 pathogenic variants [18]. The patient with MSH2 pathogenic variant had a maternal history of endometrial and colon cancer, suggesting the possibility of developing Lynch syndrome. The c.256G>T (p.Glu86*) variant in MSH2 is novel and was classified as pathogenic according to the ACMG guidelines [15].
The PMS2 gene is also an MMR gene; the PMS2 protein helps correct errors created during DNA duplication. Approximately 2% of Lynch syndrome families with pathogenic variants have a variant in PMS2 gene [19]. The nonsense variant detected in this study, c.1687C>T (p.Arg563*, rs587778618), is classified as pathogenic in the ClinVar database (http://www.ncbi.nlm.nih.gov/clinvar/) [202122].
Checkpoint kinase 2 (CHEK2) is a serine/threonine kinase that is activated on DNA damage and is involved in pathways that activate DNA repair, cell cycle arrest, or apoptosis in response to initial damage [23]. The loss of kinase function has been correlated with different cancer types, mainly breast cancer [23]. The CHEK2 gene is affected by missense or deleterious pathogenic variants. To the best of our knowledge, the CHEK2 c.546C>A variant (p.Tyr182*, rs200917541) is not included in any population databases.
The splicing site variant of the PALB2 gene (c.3351-1G>C) is classified as pathogenic (PVS1, PM2, and PP3). The Partner and localizer of BRCA2 (PALB2) protein interacts with both BRCA1 and BRCA2, forming a “BRCA complex”, in which PALB2 acts as a bridge between BRCA1 and BRCA2. Pathogenic variants in the PALB2 gene are associated with breast, pancreatic, and, possibly, ovarian cancers [242526].
Additionally, we identified a breast cancer patient with a missense variant in the MLH1 gene (c.1937A>G p.Tyr646Cys, rs35045067). This variant is classified as “uncertain significance” in ClinVar, and is not reported in the Korean reference genome database (KRGDB: http://152.99.75.168/KRGDB/). However, the patient has a significant family history (father: prostate cancer, brother: pancreatic cancer, sister: sarcoma). Thus, further family studies are needed to determine whether this variant is pathogenic or not. The MLH1 gene is another MMR gene implicated in Lynch syndrome. The inclusion of breast cancer within the syndrome remains controversial. Harkness, et al. [27] reported that female MLH1 carriers appear to be at moderate risk of breast cancer and should be considered for breast screening. Scott, et al. [28] also showed a significant increase in breast cancer cases in an MLH1 pathogenic variant-positive group. Woo, et al. [29] have stated that missense variants in MMR genes should be interpreted with caution and that multiple analyses, including functional analyses, are needed. Thus, further studies, including functional analyses, are needed to refine the clinical significance of this variant and its association with Lynch syndrome.
Our results and previous results demonstrate that there is no prognostic difference between HBOC patients with and without germline variants of cancer-related genes. Nevertheless, it would be worthwhile to determine the prognostic impact of cancer-related pathogenic variants through a large-cohort study.
Breast or ovarian cancer patients with related pathogenic variants have a family history of not only breast or ovarian cancer but also colon cancer, pancreatic cancer, prostate cancer, and sarcomas. Thus, multi-gene panel testing may be a good screening tool in such patients with a family history of cancer.
Our study has several limitations. First, family history was not collected sufficiently. To apply NCCN guidelines precisely, information on at least the 2nd degree family history of patients should be available. Due to the lack of information, some patients might have been misclassified. Second, we did not evaluate all the VUS detected in the multi-gene panel testing. Further evaluation of VUS might affect the prevalence data for the pathogenic variants in HBOC patients.
In conclusion, the NGS multi-gene panel testing demonstrated significant clinical validity in HBOC patients as a screening tool, especially for patient with a family history of cancer. The identification of women with pathogenic variants in cancer-related genes may have important implications for family testing.
 XML Download
XML Download