

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Usually fungal infections caused by opportunistic and pathogenic fungi were an important cause of morbidity and mortality among in patients having severe basic internal diseases, and also the sufferers did not have any characteristic significant symptoms. And the epidemiology, transport, and pathogenic mechanisms had not been well known. Historically the development of mycosis had been depended primarily on the immune defense competence of the patients. In addition, the clinical pictures of immunocompromised mycotic infections had been different with one another and investigative studies had been diversely accumulated hitherto. However, pathogenic fungal infections in an immunocompetent had been rare and neglected into clinical studies. Especially Cryptococcal brainstem abscess mimicking brain tumors had been also much more rare maybe due to blood brain barrier competence and indolent characteristics of such infections in an immunocompetent.
CASE REPORT
Clinical presentation
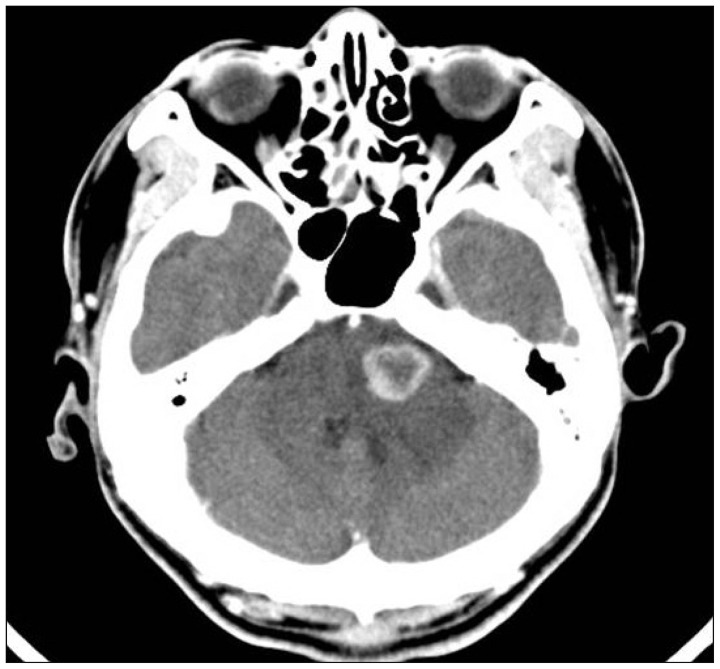
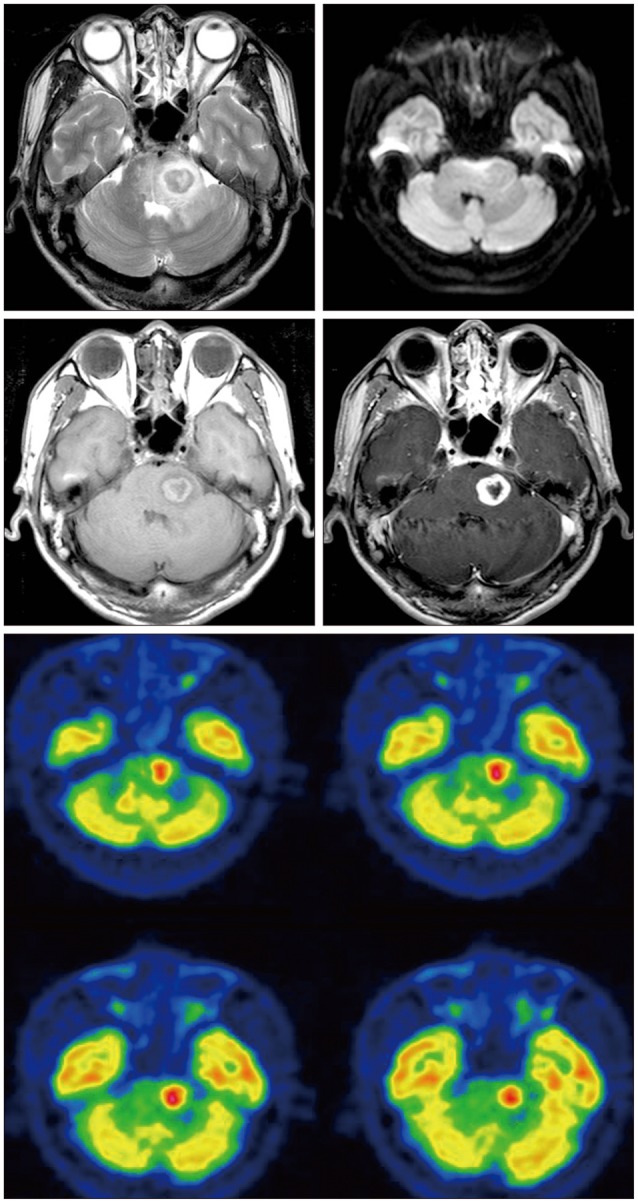
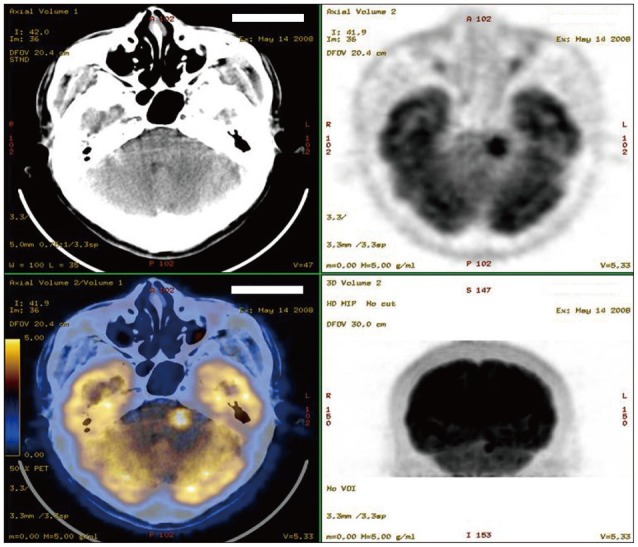
This 47-year-old man presented with a history of progressively worsening headache and nausea for 1 month and several days of vomituritions before admission. Neurological and laboratory examinations demonstrated no abnormal findings. Previously he was healthy and did not have any other significant medical diseases. A computed tomography (CT) scan revealed enhancing mass lesion with central necrosis and peripheral edema in the left pons compressing the fourth ventricle (Fig. 1), and subsequent simple, diffusion, and perfusion MRI demonstrated a rim-enhancing about 1.8×1.7×2.0 cm sized, highly perfusing mass lesion with heterogeneous low or iso-signal intensity (Fig. 2), and also positron emission tomogram (PET) scans of the whole body comprising brainstem demonstrated a hot uptake of fluorodeoxy-glucose (FDG) on the brainstem lesion without having any evidences of systemic metastasis (Fig. 3).
Operative and postoperative course
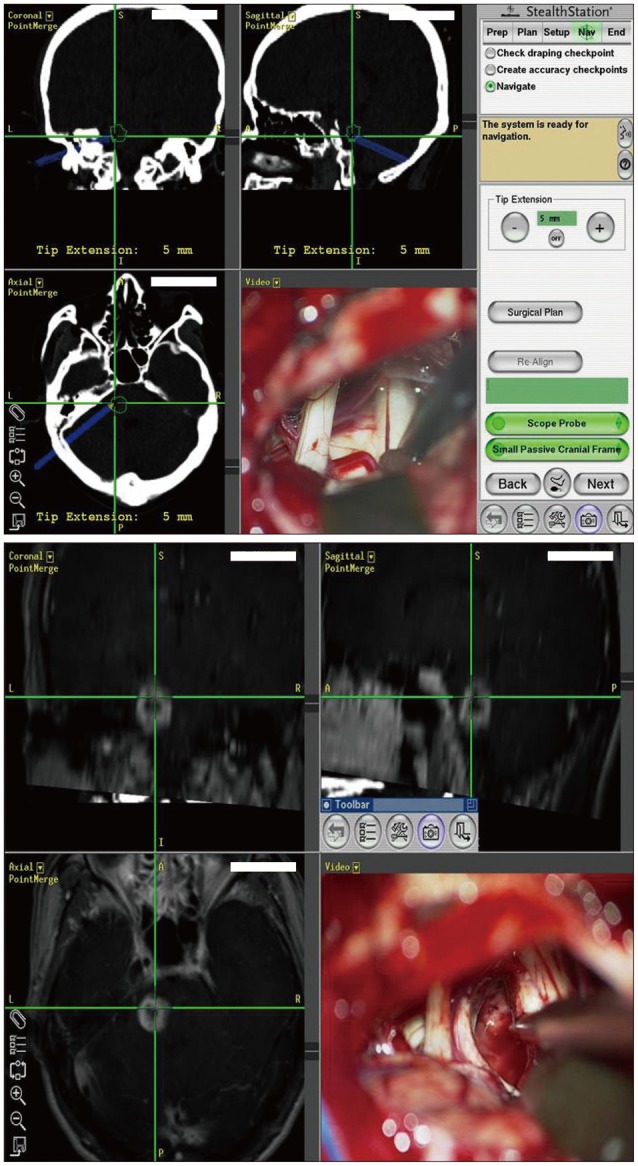
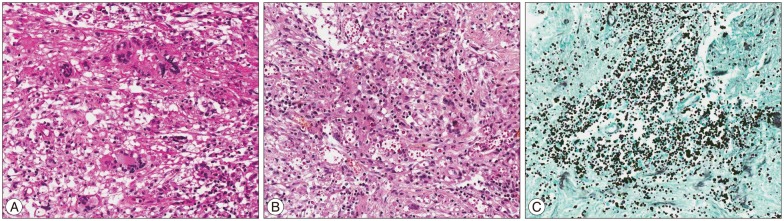
Gross total mass resection was achieved with lateral suboccipital approach with the help of neuronavigation system and somatosensory evoked potential monitoring (Fig. 4). Postoperatively he recovered without having any neurological deficits. Pathologic report confirmed Cryptococcus neoformans (Fig. 5) and the patient was successively treated with Amphotericin antifungal medications.
DISCUSSION
Cryptococcus neoformans is a medically important encapsulated pathogenic yeast often responsible for potentially life-threatening meningoencephalitis in humans. Cryptococcosis occurs world wide, and its incidence has increased with the onslaught of the human immunodeficiency virus/acquired immunodeficiency syndrome pandemic. In nature, Cryptococcus (C.) neoformans exists in two biochemically distinguishable varieties, C. var. neoformans and C. var. gatti, and also is subdivided into 5 serotyes : A, D, AD, serotypes corresponding to C. var. neoformans, and another B and C serotypes, corresponding to C. var. gatti. Differences among the specific serotypes are based on the antigenic differences resulting from structural variations of the major capsular polysaccharide glucuronoxylomannan. The specific serotypes of clinical cryptococcal isolates can be correlated with differences in epidemiology, pathogenesis, clinical presentations and patient management9). C. neoformans is an opportunistic fungus that typically affects patients who are HIV-positive and other patients with compromised immune systems. Disseminated disease may occur in up to 62% of HIV-seronegative patients with cryptococcosis2). These fungi are present in the air, on medical objects and instrumentations, in the respiratory tract and on the hands of hospital staff, and so transplantations have been the most frequent risk factors7). Cryptococcus neoformans infections usually presents as a meningitis with T-lymphocyte defects but not as a cerebral mass lesion3). However, Cryptococcal mass lesion (cryptococcoma) rarely occurred even in apparently immunocompetent child in one series4). In a diagnostic study we performed perfusion-weighted MR imaging, Hakyemez et al.7) previously reported 105 patients with lesion [high-grade glioma (n=23), low-grade glioma (n=11), meningioma (n=23), metastasis (n=25), hemangioblastoma (n=6), pyogenic abscess (n= 4), schwannoma (n=5), and lymphoma (n=5)]. The regional cerebral blood volume (rCBV) ratio of the lesions were obtained by dividing the values obtained from the normal white matter. The rCBV ratio was 5.76 in high-grade glioma, 8.02 in meningioma, 5.27 in metastasis, 11.36 in hemangioblastoma, 0.76 in abscesses, 1.10 in lymphoma, and 3.23 in schwannomas. In conclusion, rCBV ratios on perfusion MRI scan can be used to discriminate various intracranial space occupying lesions by comparing vascularities. With this rCBV tool we can discriminate between ring enhancing abscess and high-grade glioma with hemorrhagic necrosis and single metastasis1). However this case did not demonstrate such specific meaningful data. Historically lesions of the pons and brachium pontis have long been considered as a difficult diagnostic and surgical challenge. A presumptive diagnosis can often be made based upon characteristic CT and MR imaging appearances therefore, patients have been treated purely on the basis of radiologic findings in the absence of a diagnostic tissue specimen. Patients are frequently administered inappropriate empirical therapy because their diagnoses were based upon clinical and radiographic impressions not on histological grounds. And surgical approaches to the pons have generally been one of the following : 1) the suboccipital approach via the fourth ventricle; 2) an approach through a retromastoid suboccipital craniectomy via the cerebellar pontine angle; 3) the subtemporal transtentorial technique; or 4) a CT-guided stereotactic suboccipital transcerebellar biopsy. The open conventional surgical methods carry inherent risks in compromised patients and are associated with a low diagnostic yield. Stereotaxic biopsy has been shown effective and consistent in obtaining diagnostic tissue samples through a transcortical frontal trajectory or by a suboccipital transcerebellar approach6). There have been only three previously reported cases of pontine biopsies obtained by the suboccipital transcerebellar method5,6). Abernathey et al.1) present 26 cases of pontine mass lesions biopsied through a suboccipital transcerebellar approach traversing the middle cerebellar peduncle. Interestingly in this series we safely performed direct gross total mass resection simply with lateral suboccipital approach with the help of neuronavigation and SSEP monitoring system. Generally immunocompromised brain abscess medication plan is Amphotericin B 0.7 mg/kg intravenous+Flucytosine 100 mg/kg per os (PO) daily for 2 weeks, then fluconazole 400 mg PO daily for 8 weeks, then fluconazole 200 mg PO daily till stable, however, we prescribed amphotericin or fluconazole 5 mg/kg PO for 2-3 mo8).
 XML Download
XML Download