

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Granular cell tumor (GCT) is a rare tumor of Schwann cell origin. While this tumor can occur anywhere in the body, in about 50% of the cases, it involves the head and neck region.(1) GCTs have been reported in the respiratory tract, gastrointestinal tract, genitourinary tract, vulva, and the breast. Although GCTs tend to involve the head and neck region, GCT of the thyroid gland is very rare, and twelve cases were previously reported in the English literature.(2345678910111213)
CASE REPORT
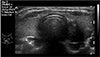
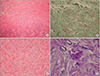
Our case is a 46-year-old woman with a medical history of right breast cancer. She underwent modified radical mastectomy of the right breast due to invasive lobular carcinoma (T1N1M0) and received six cycles of CAF (cyclophosphamide, adriamycine and 5-flurouridine) combination chemotherapy. While receiving chemotherapy, follow-up breast & thyroid ultrasound were performed, revealing a 1.5×1.6×2.1 cm nodule in the left thyroid (Fig. 1). The nodule was an ill-defined solid, ovoid to round in shape, heterogeneous and hypoechoic. The subsequent ultrasound-guided fine needle aspiration cytology (FNAC) was benign category in the Bethesda System for reporting thyroid cytology. A follow-up ultrasound of the thyroid performed 4 months later showed little interval change and the ultrasound-guided FNAC was unsatisfactory. The patient complained of voice change after the FNAC, so underwent operation. On surgical findings, tumor was located in the posterolateral aspect of the lower pole of the left thyroid and infiltrating into surrounding thyroid tissue and muscles, with suspicious of a malignant nature. It was also found to have encased a portion of the recurrent laryngeal nerve, while abutting the trachea and the esophagus. The lobectomy of the left thyroid was performed with preserving the recurrent laryngeal nerve. Frozen-section pathologic result performed during the operation couldn't confirm malignancy, so further operation was not performed. The cut sections of the tumor showed that it was ill-demarcated, 2.4×1.7 cm in size, whitish and fibrotic, while seeming to involve the capsule of thyroid gland. Histologic findings showed a tumor with ill-defined margins, consisting sheets of large polygonal cells separated by dense fibrous tissue (Fig. 2A, B). The tumor cells had small hyperchromatic nuclei with abundant eosinophilic and granular cytoplasm (Fig. 2C). The cytoplasmic granules were periodic acid Schiff (PAS)-positive (Fig. 2D). Immunohistochemically, they showed positive reaction for S-100 protein (Fig. 3A), neuron-specific enolase (Fig. 3B), and vimentin and negative reaction for cytokeratin and desmin. Ultrastructural feature showed abundant lysosomes having lamellate appearance and fragmentation in the cytoplasm (Fig. 3C). According to histologic and immunohistochemical findings, we finally diagnosed this case as the granular cell tumor of thyroid. The patient was tolerable after operation, and her voice was recovered during several weeks after operation.
DISCUSSION
GCTs, originally described as granular cell myoblastomas, are benign, soft tissue tumors which can occur in many locations, such as tongue, skin, subcutaneous tissue, breast, esophagus, stomach, and larynx.(813) The skin of the trunk and tongue are most common site and GCTs of thyroid are very rare. GCT can occur in patients of all ages, but most commonly in middle-aged woman of 40 to 50 years old. GCTs are usually solitary, 10~15% are multifocal with involving one or several organs or tissues. Twelve cases have been reported in the English language literatures and summarized in Table 1.(2345678910111213) Most of the patients reported were female, except one patient and between 11 and 47 years old. It presents most commonly as a painless, single nodule, but the location of the tumor determines whether or not the tumor causes symptoms. The size of tumors are 8~42 mm in reported tumors. On ultrasound and gross findings, GCTs can be suspicious with malignancy, because the tumors are usually ill-defined marginating and infiltrating into surrounding tissues. Also, it is difficult to diagnose a GCT before surgery by FNAC. The preoperative FNAC in six cases of previously reported ones showed that tumor cells were large in shape, syncytial, with abundant eosinophilic granular cytoplasm and indistinct order, and nuclei of the cells were polymorphic, presenting in round, oval, or spindle shapes.(8910111213) The differential diagnoses of GCT, which should be considered via preoperative FNAC, were following diseases and cell types; Hurthle cell tumor and dysplastic nodules, macrophages with high nuclei-cytoplasm ratio in benign follicular nodular cystic changes, cells of the eosinophilic subtype of medullary thyroid carcinoma, non-neoplastic follicular cells, and rhabdomyoma cells.(13) Histologically, the periphery of the tumor is not sharply defined and detached groups of granular cells may extend away from the main tumor, creating an appearance of infiltration. This is a characteristic histological feature of GCT and therefore should not be considered as malignancy.(1) GCTs are usually benign and only 1~2% have been reported to be malignant. Malignant GCT is rare and rapid growing tumor with diameter larger than 5 cm. Criteria for malignancy in GCT include six histologic features; necrosis, prominent spindled pattern, nuclear pleomorphism, vesicular nuclei with large nucleoli, increased mitotic activity (more than 2 mitoses/10 high-power fields at 200× magnification), high nuclei-cytoplasm (N : C) ratio.(14) Tumor including three or more of these criteria was classified as histologically malignant; that including one or two criteria as atypical; and that including only focal pleomorphism as benign. Malignant granular cell tumor is a high-grade sarcoma with a high rate of metastases and a short survival. The statistically-significant poor prognostic factors associated with survival were local recurrence, metastasis, large tumor size, older patient age, histologic classification as malignancy, presence of necrosis, increased mitotic activity, spindling of tumor cells, vesicular nuclei with large nucleoli, and Ki67 values less than 10%. In our case, even though the tumor has invaded the thyroid tissue and the recurrent laryngeal nerve, explaining the patient's voice change, it was benign. GCT in thyroid should be differentiated with all other oncocytic/Hurthle cell neoplasm and medullary carcinoma. The immunohistochemical stains can confirm the final diagnosis of GCT and differentiate other pathologic changes from GCT. Immunohistochemistry showed that the tumor cells were positive for S-100 protein, vimentin, CD68, and other neural markers such as neuron-specific enolase (75~100%), PGP 9.5 (100%), whereas negative for thyroglobulin, thyroid transcription factor-1, and calcitonin.(1) The treatment of choice for GCT is surgery and benign GCTs rarely recur if completely resected, with excellent prognosis.


 XML Download
XML Download