

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sports related injuries account for significant number of traumatic spinal injuries. Especially, golf stresses the body in unique ways that can lead to acute and chronic spinal injuries. In golf, the mechanism of the cervical injury is similar to that of occupational Clay-shoveler's fracture. Clay-shoveler's fracture represents an avulsion type of fracture of the spinous process in the lower cervical or upper thoracic spine. Here, we'll report the case of a sports-related cervical spinous process fracture with a discussion on the causative mechanism, treatment and prognosis.
Case Report
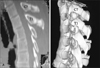
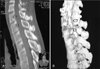
A 37-year-old man had a sudden lower posterior neck pain. During the physical examination, he complained about severe tenderness between both shoulder blades, limitation in range of neck motion, and a cracking sound in the painful posterior cervico-thoracic junction. This symptom happened during his golf swing. He has been an amateur golfer for the past two months. He had been swinging his driver almost everyday before symptoms occurred. A Neurologic examination was normal. Initial cervical spine X-rays showed an isolated spinous process fracture C-7 vertebra (Figure 1). In the lateral dynamic flexion-extention views, the bone fragments and vertebral body were not mobile and stable. A computed tomography showed an additional T-1 spinous process fracture (Figure 2). He was prescribed analgesics and muscle relaxants. Cervical immobilization was done for 4 weeks with a cervical collar brace. After one year, the patient revisited our institute with posterior neck pain and tenderness, pre-described similar symptoms. But the intensity of the pain was relatively softer than the previous one-year ago symptom. Neurological examinations were normal. A computed tomography showed a multiple isolated cervical and thoracic spinous process fractures (Figure 3). It ranged from the C-7 to T-4 vertebra. He had been golfing again for the past one year. The patient was managed in the same ways. Three years later, he visited our clinic again due to transient neck discomfort. We evaluated him with a computed tomography (Figure 4). This showed a complete union from the T-2 to T-4 but malunion on C-7 and T-1. These are more mobile segments. Later, He was discharged and recommended to perform physical therapy.
Discussion
The pathomechanism of golf-related cervical spinal fracture is very similar to so called "Clay-shoveler's fracture".1,2) It is known as an occupational injury which occurs when workers shovel heavy loads for a long time. This type of fracture has been increasingly seen in sports-related injuries, especially golf, wrestling and cricket, etc.3) The cervicothoracic junction is the main target, especially between C-7 and T-1.1,4) It is suggested that the causation of golf-related injuries is closely associated with origins and actions of trapezius, the rhomboideus major, the rhomboideus minor and the serratus posterior muscles.5) It seems that there are five possible mechanisms by which this fracture may be explained:
1) Direct muscle violence by direct pull of the muscle.
2) Reflex muscle contraction.
3) Whip-like pull transmitted through the supraspinal ligaments.
4) Indirect cervical hyperextension and hyperflexion avulsion.
5) Muscle and ligament stress that result in a fatigue fracture.
The complex motions of such type of fracture have been described in details, first by Le Baron and then by Sicard and Carrage.6-8) In the present case, it was from complex of above multiple mechanism. The first is the indirect true avulsion-type fracture by counterforce between the thoracic cage and cervicothoracic junction. The second may be regarded as a stress-related, fatigue-type fracture. The fracture line is usually located in the middle of the spinous process which are the most weakest point in the spinous process.1) The distal fragment is usually displaced downward and laterally (Figure 1). The two ends are often widely separated, and as a result, nonunion is common. The most useful imaging study for a cervical spine fracture is radiography. A double spinous process shadow at the affected level can be detected from antero-posterior views.2) Downward displacement of the fractured bone fragment can be seen in lateral views (Figure 1).1,9) These radiologic findings are differentiated from the calcification of ligamentum nuchae, absence of the secondary ossification center, and osteochondritis of the spinous process in adolescence, or Schmitt's disease.10)
The most common symptom of the isolated spinous process fracture is pain which sometimes radiates up to the head and down both shoulders. A physical examination may reveal tenderness in the posterior neck and it is possible to hear a cracking sound in that region. Generally, neurological signs and symptoms may be normal but it is considered carefully with additional spinal injuries. The multiple isolated cervical spinous process fractures are a benign condition that often resolves itself spontaneously. In most patients, immobilization of the neck by means of a collar and restriction of physical activity for 4 to 6 weeks frequently results in pain relief.
Conclusion
This paper describes a case of multiple isolated cervical spinous process fractures with successive progression to the adjacent vertebra. Unless there is an appropriate management, including cessation of causative action movement, the golf-related spinous fracture may affect to additional adjacent vetebra level. Most of these types of fracture can be controlled conservatively.


 XML Download
XML Download