

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Ginseng has been a long historical traditional medicine in the Eastern countries, and the pharmacological effects of ginseng have been demonstrated in central nervous systems, cardiovascular, endocrine, and immune systems.[1] Much evidence suggests that ginseng can be effective in reducing learning deficits and memory impairment due to brain damage or aging in rodents.[2345678910] Furthermore, ginseng increases choline acetyltransferase levels in the rodent brain,[111213] and significantly increases long-term potentiation (LTP).[1415] Neuroprotective properties of ginsenosides have also been demonstrated in vitro and in vivo.[216] Thus, the favorable effects of ginseng on the general brain function were demonstrated by numerous publications and animal studies.
Although several studies demonstrated that ginseng improves cognitive function in the rodent,[217] there are only a few clinical studies about cognitive improvement effect of chronic ginseng treatment currently. Two clinical studies reported that ginseng or red ginseng has good cognitive improvement effects in Alzheimer Disease (AD) patients as a supplementary treatment.[1819] Despite that, some contrary reports suggested that evidence is scarce for the efficacy of ginseng as an effective treatment in geriatric or AD patients.[2021] There is much evidence that supports the benefits of ginseng as a medication for brain function, and more research is in progress.
In the present study examining whether ginseng has a cognition-enhancing function in Korean subjects who have mild cognitive impairment (MCI), a randomized, double-blind, placebocontrolled clinical trial was conducted.
Methods
Preparation and characterization of ginseng
Panax ginseng (4-year-old Panax ginseng) was kindly supplied by the Chungbuk Ginseng Cooperative Association (the ginseng contains total 53 mg/g ginsenoside) powdered and encapsulated (300 mg/1 capsule) by HANIL PFC. Co., Ltd.
Participants
Ninety Korean subjects aged 50 to 75 years and have MCI were enrolled in the study. MCI was diagnosed according to the criteria proposed by Petersen et al.[22] To exclude the AD patients, the Korean version of MMSE (K-MMSE) score of all subjects who were allowed to enroll was required to be over 26 points.
All subjects underwent an extensive clinical evaluation including physical and neurological examination, laboratory tests, and neuropsychological tests. Exclusion criteria were a current or past diagnosis of a somatic, psychiatric, neurological disorder that may have caused the cognitive impairment such as stroke, transient global amnesia, normal hydrocephalus, Parkinson's disease, head trauma, brain tumor, a history of alcohol or substance abuse, thyroid disease, or depression. In addition, participants who took medications that affect cognition were excluded. Furthermore, the written informed consent was obtained from each subject.
Study design
A randomized, double-blind, placebo-controlled clinical trial was conducted at a single center (Kyung Hee Medical Center) from May 2009 to April 2010. A total of 172 volunteers participated in the screening examination, and 90 were enrolled in the present study. After randomly assigning the subjects to the ginseng group (n = 45) or placebo group (n = 45), the subjects of each group were administrated Panax ginseng powder (3.0 g/day) or placebo (3.0 g/day of starch) for 24 weeks. All subjects were visited at the initial screening, baseline, 8 weeks, 16 weeks, 24 weeks, and follow up period.
The study protocol was approved by Institutional Review Broad (Kyung Hee University Hospital, Seoul, Republic of Korea) and the clinical trial was conducted in accordance with the principles of International Conference of Harmonization for Good Clinical Practice and the ethical standards for human experimentation established in Declaration of Helsinki.
Evaluation of cognitive function and safety
K-MMSE, the Korean version of Instrumental Activities of Daily Living (K-IADL), and Seoul Neuropsychological Screening Battery (SNSB) were used to assess the changes in cognitive function.[23] K-MMSE was done at baseline (screening period), 16 weeks and 24 weeks; K-IADL was done at baseline (day 1), 16 weeks and 24 weeks; SNSB was done at baseline (day 1) and 24 weeks. The SNSB, an extensive neuropsychological battery test that covers multiple cognitive subsets includes the following five specific domains: attention, language, visuospatial function, memory, and frontal executive function; attention (forward and backward digit span and letter cancellation test), language and related functions (reading, writing, comprehension, repetition, confrontational naming using the Korean version of the Boston Naming Test [KBNT], finger naming, right and buccofacial praxis tests), visuospatial function (the Rey Complex Figure Test [RCFT]; copying), verbal memory (Seoul Verbal Learning Test [SVLT]; immediate recall, 20-min delayed recall and recognition), visual memory (the RCFT; immediate recall, 20-min delayed recall and recognition), and frontal executive function (motor impersistence, contrasting program, go-no-go test, fist-edge-palm, alternating hand movement, alternating square and triangle, luria loop, phonemic and semantic Controlled Oral Word Association Tests [COWAT], and the Korean version of the Stroop Color and Word Test).
For safety evaluation, vital sign (systolic and diastolic blood pressures, pulse rate), laboratory test (complete blood cell count, chemistry laboratory test, thyroid-stimulating hormone, urinalysis), and adverse event were checked for subjects. Vital signs were checked at every visit time (6 times); Laboratory test was done at screening period, 16 weeks, 24 weeks, and follow up period.
Statistical analysis
A total of 90 subjects were finally determined according to the anticipated dropout rate of 20%, resulting in 72 subjects (36 per group). The sample size would enable a mean difference of 2 for the delayed recall score between both groups to be detected, assuming 80% power at the significance level of 5% (two-sided). The delayed recall scores were 4.32 ± 3.23 (mean ± SD) in the MCI group and 5.71 ± 2.21 in the control group according to the medical records from the outpatient clinic of Kyung Hee Medical Center. Therefore, the variance of delayed recall score for the MCI group was assumed as 32.
Data are shown as mean ± Standard Deviation (SD) or as numbers (percentage). Efficacy analyses were primarily performed on a per-protocol (PP) basis, with intention-to-treat (ITT) analysis used additionally. Adverse events assessment was also performed on PP analysis and additional ITT analysis. Intergroup comparisons for changes from baseline in K-MMSE, K-IDAL, and SNSB scores were performed by two-sample t-test. Intergroup comparisons for changes from baseline in vital sign and laboratory test were also performed by two-sample t-test.
Repeated measures analysis of variance was performed with ANOVA in order to compare the changes of K-MMSE and K-IADL in two groups as the time progressed. Therefore, we checked K-MMSE and K-IADL scores at 16 weeks and 24 weeks additionally. Null hypotheses of no difference were rejected if p-values were less than 0.05. All analytical data were obtained by using the SAS program (Ver. 9.2, SAS Institute Inc., Cary, North Carolina, USA).
Results
Participant characteristics
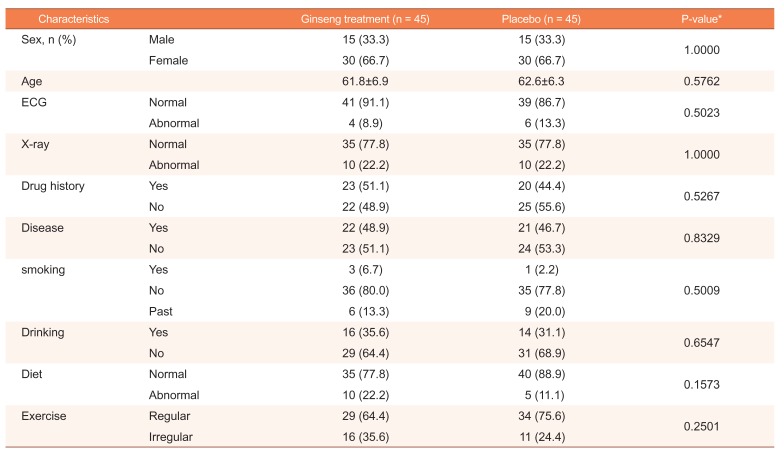
Ninety subjects were enrolled in the study (aged 50 to 75 years), and were randomly assigned to ginseng group (n = 45, male = 15, female = 30, mean age = 61.8 ± 6.9) or placebo group (n = 45, male = 15, female = 30, mean age = 62.6 ± 6.3). Baseline and demographic characteristics for all participations are summarized in table 1. A total of 82 subjects (ginseng group = 41, placebo group = 41) completed all 24 weeks of study. There were no significant differences between two groups in baseline characteristics which included age, sex, ECG, X-ray, drug history, diseases, smoking, drinking, diet habit and exercise habit (Table 1).
Changes in cognitive function
Baseline characteristics for efficacy analysis including K-MMSS, K-IADL and SNSB scores on both PP and ITT scores showed no differences between ginseng and placebo groups (P > 0.05). After 24 weeks, the changes from baseline in K-MMSS, K-IADL, SVLT immediate recall, and 20-min delayed recall scores showed no significant differences between groups.
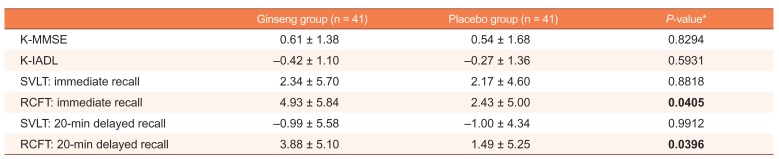
In the efficacy analysis on PP basis, changes from baseline to 24 weeks in RCFT immediate recall score (visual learning) were 4.93 ± 5.84 (ginseng group) and 2.43 ± 5.00 (placebo group). Changes in RCFT 20-min delayed recall scores (visual memory) were 3.88 ± 5.10 (ginseng group) and 1.49 ± 5.25 (placebo group). There were statistically significant differences in changes of RCFT immediate recall and 20-min delayed recall scores between the ginseng group and placebo group (P = 0.0405, P = 0.0396, two sample t-test) (Table 2).
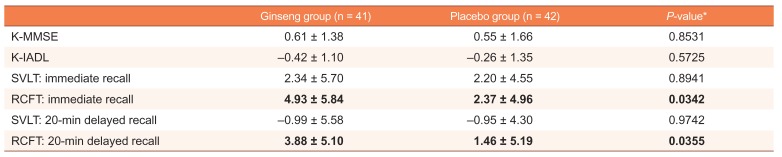
In the efficacy analysis on ITT basis, changes from baseline to 24 weeks in RCFT immediate recall score were 4.93 ± 5.84 (ginseng group) and 2.37 ± 4.96 (placebo group). Changes in RCFT 20-min delayed recall scores were 3.88 ± 5.10 (ginseng group) and 1.46 ± 5.19 (placebo group). There were statistically significant differences in changes of RCFT immediate and 20-min delayed recall scores between the ginseng group and placebo group (P = 0.0342, P = 0.0355, two sample t-test) (Table 3).
In the repeated measures analysis, there were no statistically significant differences in K-MMSE and K-IADL between ginseng group and placebo group over time (P = 0.3197, P = 0.8842, ANOVA) (Table 4).
Adverse events and safety assessment
There were three cases of adverse events, two cases from the ginseng group and one case from the placebo group during 24 weeks administration. One subject from the ginseng group showed a mild increase in thyroid-stimulating hormone (TSH) at the end of the trial. Another subject from placebo group also showed a moderate increase in TSH during the trial. One subject from the ginseng group underwent polypectomy during the trial. None of these adverse events were related to ginseng administration. These adverse events were mild or moderate and transient.
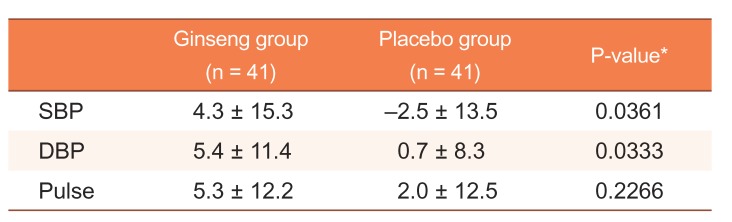
In vital sign, changes in systolic blood pressure (SBP) from baseline to 24 weeks of two groups were 4.3 ± 15.3 for the ginseng group and −2.5 ± 13.5 for the placebo group. There was a statistically significant difference between two groups (P = 0.0361, two sample t-test). Changes in diastolic blood pressure (DBP) from baseline to 24 weeks of two groups were 5.4 ± 11.4 for the ginseng group and 0.7 ± 8.3 for the placebo group. There was a statistically significant difference between two groups (P = 0.0333, two sample t-test). Pulse did not show statistically significantly different in change from baseline to 24 weeks (P = 0.2266, two sample t-test) (Table 5). In laboratory test results, there were no statistically significant changes from baseline to 24 weeks.
Discussion
We performed a randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of Panax ginseng in Korean volunteers with MCI and found that Panax ginseng treatment improved cognitive performance in subjects with MCI.
A number of experimental studies have suggested that ginseng improves the cognitive function in rodents.[217] However, there were few clinical studies demonstrating cognition enhancement effects of ginseng. Lee et al. suggested that as an additional treatment, 12 weeks ginseng treatment (4.5 g/day) enhanced cognitive function in AD patients.[18] They also reported that the improvement of cognition by ginseng treatment disappeared after the ginseng withdrawal.[18] Heo et al. also suggested that Korean red ginseng as an adjuvant therapy has positive effects on cognitive improvement in AD.[19] However, according to the systematic review by Lee et al., the evidence of ginseng's efficacy in AD patients was scare and inconclusive.[21] Also, a double-blind, controlled clinical trial reported that there was no improvement in geriatric patients on the performance of the MMES.[20] Although some studies reported acute effects of ginseng on cognitive performance in healthy volunteers,[242526] there were few studies demonstrated that chronic ginseng treatment had improved the cognitive function in subjects who have MCI currently.
Therefore, we used a randomized, double-blind, placebocontrolled method that is different from the previous two openlabel studies.[1819] The ginseng group were showed significant improvement in RCFT immediate recall (P = 0.0405 on PP analysis, P = 0.0342 on ITT analysis) and RCFT 20-min delayed recall (P = 0.0396 on PP analysis, P = 0.0355 ITT analysis) scores compared with placebo group, and such results suggested that visual memory function (visual learning and visual memory) of subjects were significantly improved after chronic ginseng treatment.
However, the ginseng group did not show significant improvement in SVLT scores, which covers verbal memory function (verbal learning and verbal memory). We conjectured that there were more ceiling effects of K-MMSE and verbal memory test than a visual memory test. Because K-MMSE scores of all subjects with MCI were over 27 points, there was no margin to detect the changes in K-MMSE scores.
Although the suggestions of several studies were different from our results, our results strongly supported the results from the previous two studies, which demonstrated the positive effect of ginseng in cognitive function.[1819] Furthermore, there was no related adverse drug event during the trial. These results showed that ginseng has cognition-enhancing effect and can be used safely.

 XML Download
XML Download