This study used cone-beam computed tomography (CBCT) images to categorize the relationships between the mandibular canal and the roots and investigated the prevalence of nerve damage.
Through CBCT images, contact and three-dimensional positional relationships between the roots of the mandibular third molar and the mandibular canal were investigated. With this data, prevalence of nerve damage according to the presence of contact and three-dimensional positional relationships was studied. Other factors that affected the prevalence of nerve damage were also investigated.
When the mandibular third molar and the mandibular canal were shown to have direct contact in CBCT images, the prevalence of nerve damage was higher than in other cases. Also, in cases where the mandibular canal was horizontally lingual to the mandibular third molar and the mandibular canal was vertically at the cervical level of the mandibular third molar, the prevalence of nerve damage was higher than in opposite cases. The percentage of mandibular canal contact with the roots of the mandibular third molar was higher when the mandibular canal was horizontally lingual to the mandibular third molar. Finally, the prevalence of nerve damage was higher when the diameter of the mandibular canal lumen suddenly decreased at the contact area between the mandibular canal and the roots, as shown in CBCT images.
The three-dimensional relationship of the mandibular third molar and the mandibular canal can help predict nerve damage and can guide patient expectations of the possibility and extent of nerve damage.
Extraction of the mandibular third molar is the most widely performed oral and maxillofacial surgery. However, one of the severe complications of this surgery is damage to the inferior alveolar nerve
Recently, cone-beam computed tomography (CBCT) has become an important tool in oral and maxillofacial radiology because it is more economic and causes less radiation exposure than conventional computed tomography (CT). Though CBCT is more expensive and causes more radiation exposure than panoramic radiography, it is applied widely due to its three-dimensional capability. In particular, when the mandibular third molar and the mandibular canal are adjacent, CBCT is able to visualize the buccolingual position, curvature and number of roots, the distance and location from the mandibular canal, the loss of cortical layer of the mandibular canal, and the direction of the mandibular canal
However, studies involving cases from which to evaluate the prevalence of nerve damage are insufficient. In addition, few studies demonstrate the prevalence of nerve damage according to the positional relationships of the two structures or the shapes of the roots or the mandibular canal.
This study discusses clinical complications experienced after extraction of the mandibular third molar from patients who had overlapping panoramic radiography views of the root of the mandibular third molar and the mandibular canal. The positional relationship between the mandibular third molar and the mandibular canal was analyzed radiographically, and the influence on the damage to the inferior alveolar nerve was also studied. Moreover, the prevalence of nerve damage according to the shapes of the roots of the mandibular canal were studied.
From 2012 to 2013, patients who visited Dankook University Dental Hospital (Cheonan, Korea) for mandibular third molar extraction were evaluated, and the patients with an overlapped panoramic radiography view of the root of the mandibular third molar and the mandibular canal were included in this study. Cases with cysts or tumors of the mandible were excluded. A total of 224 CBCT images of the mandibular third molar were included in this study. The institutional review board of Dankook University Dental Hospital approved the design of this retrospective cohort study.
The CBCT machine used in this study was a PHT-60FO model (VATECH Corp., Hwaseong, Korea), and mandibular third molars were exposed at 80 kV and 2 mA for 17 seconds. Images were processed using 3DX software (Mortita, Kyoto, Japan) and evaluated through light emitting diode monitors.
The following aspects were investigated using the CBCT images of 224 mandibular third molars: (1) Impaction depth (partial or entire), (2) number of roots (1, 2, >2), (3) shape and curvature of mesial and distal roots (straight, buccal, lingual, distal, mesial), (4) proximity of the roots and the mandibular canal, and (5) horizontal and vertical positional relationships between the roots and the mandibular canal.
To determine how contact between the roots of the mandibular third molar and the mandibular canal influenced the prevalence of loss of sensory nerve function, two groups were created according to the CBCT images: group 1, no contact between the roots of the mandibular third molar and the mandibular canal, with a separating cortex layer; group 2, contact between the roots of the mandibular third molar and the mandibular canal, without a separating cortex layer.
Logistic regression analyses were used for statistical purposes. The results were statistically significant when the
The relationships between the roots of the mandibular third molar and the mandibular canal, based on CBCT images, were used to evaluate nerve damage prevalence according to the horizontal and vertical positions. The location of the mandibular canal to the mandibular third molar was categorized horizontally (buccal, apical, lingual) and vertically (apical one-third, middle one-third, cervical one-third). The prevalence of nerve damage according to the positional relationships was investigated. The Pearson chi-square test was used for statistical purposes.
The buccolingual relations of the roots of the mandibular third molar and the mandibular canal and the contact between the mandibular third molar and the mandibular canal were studied to investigate the variations in the prevalence of nerve damage according to the buccolingual position of the mandibular canal based on CBCT images. Fisher's exact test was used for statistical analysis.
Tooth-related variables and nerve canal-related variables were studied separately to investigate other variables that caused nerve damage when there was direct contact between the mandibular third molar and the mandibular canal.
Tooth-related variables included age, gender, and buccal or oral bending of the distal root. Nerve canal-related variables included age, gender, diameter of the canal lumen, root bending inside the canal, and contact area between the root and the canal. IBM SPSS Statistics version 19.0 (IBM Co., Armonk, NY, USA) was used for statistical analysis.
The results of impaction depth, number of roots, shape and curvature of mesial and distal roots, proximity of the roots and the mandibular canal, and horizontal and vertical positional relationships between the roots and the mandibular canal from 224 mandibular third molars based on CBCT were as follows. The majority of teeth were partially impacted and had two roots. Twenty-one teeth (9.3%) had their distal roots curved in the buccolingual direction, and 71 teeth (31.7%) were in contact with the mandibular canal. Finally, the mandibular canal tended to be on the buccal side (48.2%) rather than the lingual side (26.3%) or at the apex (25.4%) relative to the roots of the mandibular third molar.(
CBCT images of 224 teeth were studied. In all, 11 teeth (4.9%) experienced nerve damage that affected the inferior alveolar nerve. Only one patient in group 1 had nerve damage, while 10 patients in group 2 experienced nerve damage in the absence of a cortex layer. The prevalence of paresthesia when the roots of the mandibular third molar contacted the mandibular canal was 21 times greater than that of cases without contact. In conclusion, the presence of contact between the two structures greatly influenced resulting nerve damage.(
The prevalence of nerve damage according to the horizontal and vertical positional relationships between the roots and the mandibular canal is shown.(
The possibility of contacting the roots was higher when the mandibular canal was located more lingual than the mandibular third molar. In 51 of the cases (71.8%) where the mandibular canal was lingually positioned, the nerve and roots had contact with each other. When the mandibular canal was buccally positioned, 17 cases (23.9%) showed no contact between the nerve and the roots. In this respect, there is an increased likelihood of contact with the nerve canal when the mandibular canal is lingually positioned, and as a result, there is a greater possibility of nerve damage.(
Other variables that caused nerve damage were studied, with the exception of direct contact between the mandibular third molar and the mandibular canal. For tooth-related variables, the possibility of nerve damage was high if the patient was aged or the distal root was curved buccolingually, but the value was not statistically significant.(
Extraction of the mandibular third molar is one of the most common oral and maxillofacial surgeries. Complications such as hemorrhage, infection, edema, trismus, alveolar osteitis, ecchymosis, and nerve damage can occur after surgery. A number of clinicians have studied if additional CBCT before mandibular third molar extraction could decrease the prevalence of postoperative complications. Susarla and Dodson
Numerous studies on the diagnostic usefulness of CBCT for mandibular third molar extraction have been reported
Maegawa et al.
Determination of the exact location of the mandibular canal illustrates the safe region for removing bone for extraction and the hazardous region that requires surgical caution
Never damage does not always occur, even when the mandibular third molar and the mandibular canal contact each other. One study reported a high prevalence of paresthesia when the diameter of the canal lumen decreases near the location of the roots of the mandibular third canal and where there is contact with the mandibular canal based on CBCT images
This study investigated the relationship of the mandibular third molar and the mandibular canal as shown in CBCT images and the correlation with postoperative complications, especially nerve damage. Even though CBCT images cannot significantly prevent complications after extractions compared with panoramic radiograph images, evaluating the contacts between the mandibular third molar and the mandibular canal using CBCT images and the changes in the diameter of the canal lumen can be effective for predicting the extent of nerve damage prior to surgery. Of the 224 teeth in this study evaluated with CBCT images, only 11 experienced temporary nerve damage. However, this is a serious complication for patients and a great postoperative burden for surgeons. Consequently, this study provides useful information for clinicians about evaluating risk factors for postoperative complications and nerve damage using CBCT images.
Panoramic radiograph images indicate that, when the mandibular third molar and the mandibular canal are in direct contact, it is critical to determine the exact positional relationship of the two structures with CBCT images. The presence of contact between the mandibular third molar and the mandibular canal in CBCT images was determined to be related to the degree of nerve damage. The frequency of roots that contacted the mandibular canal was higher when the mandibular canal was lingual to the mandibular third molar, and consequently, the prevalence of nerve damage was higher. Additionally, the analysis indicated that a decrease in the diameter of the canal lumen at the contact area affected the prevalence of nerve damage. In conclusion, CBCT can be valuable for determining the three-dimensional relationship of the mandibular third molar and the mandibular canal; this can allow operating surgeons to explain the possibility and extent of nerve damage to prospective patients.
The present research was conducted by the research fund of Dankook University in 2014.
No potential conflict of interest relevant to this article was reported.
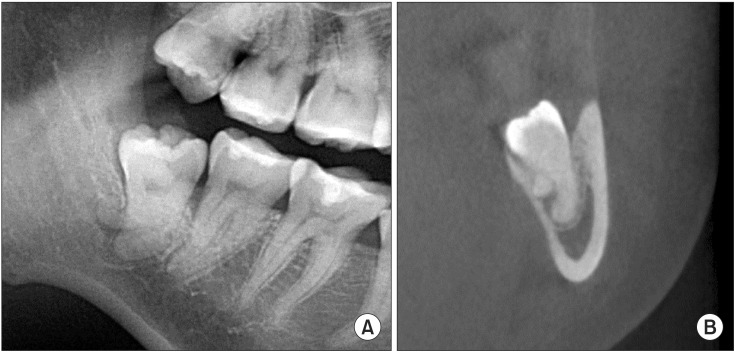
Radiographic images of a patient with paresthesia. A. A panoramic radiographic image shows the roots of the mandibular third molar overlapping the mandibular canal. B. The roots show lingual bending, and the continuity of the canal of the inferior alveolar nerve is lost.
Distribution of tooth-related variables as observed in cone-beam computed tomography in relation to surgical interventions (n=224)
(IAC: inferior alveolar canal, MTM: mandibular third molar)
Prevalence and relative risk of paresthesia according to the cortical integrity of the inferior alveolar canal (IAC)
Relative risk, 21.5; 95% confidence interval, 2.7-157.
Group 1: no contact between the roots of the mandibular third molar and the mandibular canal, with a separating cortex layer. Group 2: contact between the roots of the mandibular third molar and the mandibular canal, without a separating cortex layer.
Prevalence of paresthesia and position of the IAC in relation to the MTM
(IAC: inferior alveolar canal, MTM: mandibular third molar)
1Pearson's chi-square test.
Relationship between the buccolingual position and proximity of the canal
1Fisher's exact test;
Multivariate logistic regression analysis for tooth-related factors for paresthesia prevalence
Multivariate logistic regression analysis for canal-related factors for paresthesia prevalence