

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
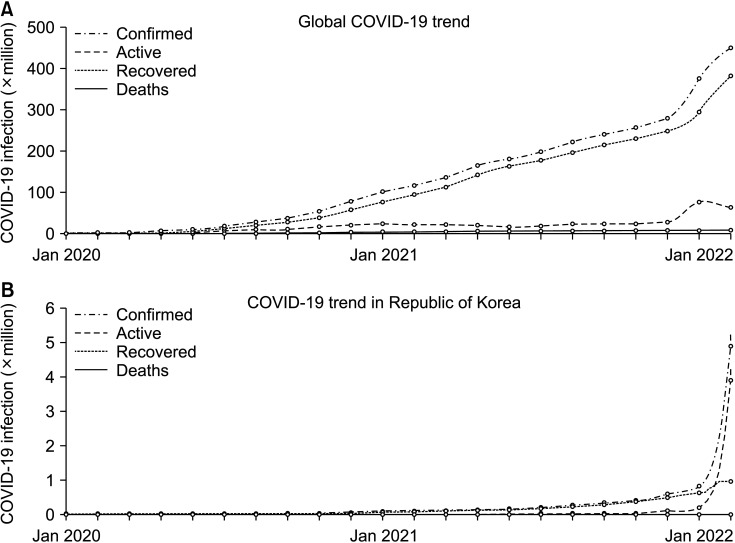
The emergence in December 2019 of a cluster of patients with pneumonia was identified to have been caused by 2019-nCoV, a novel coronavirus [1], which was later classified as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [2]. This coronavirus (now referred to globally as coronavirus disease 2019 [COVID-19]) was subsequently announced to be the cause of a global pandemic by the World Health Organization (WHO) on March 11, 2020 [3]. In the 2 years since then, over 452 million cases of COVID-19 have been documented accounting for more than 6 million deaths. Although over 60% of the world’s population has now received a COVID-19 vaccine, around 1 million new cases and 7,000 deaths are still being recorded each day due to this virus. Moreover, the recent dramatic increase of daily COVID-19 patients in the Republic of Korea accounts for almost 30% of the daily new cases being reported worldwide (Fig. 1) [4].
The impacts of COVID-19 have been globally paradigm shifting in all aspects of people’s daily lives. From a clinical perspective, surgeons have also experienced unprecedented changes due to this pandemic regarding operation schedules, preparations before surgery, and the precautions needed both during and after surgery. Prior experiences with Middle East respiratory syndrome and SARS-CoV have helped with this to some degree, but the magnitude of the spread of COVID-19 has been incomparable in this regard [5]. A global expert response study was conducted just after the declaration of the pandemic in an effort to estimate the worldwide cancellation of surgeries that would occur. This study included all 193 United Nations member countries except Liechtenstein, North Korea, and Somalia. The number of canceled surgeries worldwide was estimated to have ranged from 19 to 43 million in the peak 12 weeks of the COVID-19 outbreak, of which the duration was wildly underestimated. More than 80% of elective surgeries and 30% of cancer surgeries were anticipated to have been canceled [6].
There were obvious concerns that necessary surgeries would not be provided in time for many patients in need and that this would have a detrimental influence on short-term survival outcomes. Cases of malignant disease were, unsurprisingly, of particular concern due to not only the delayed surgery but also the postponements of surveillance or regular check-ups. Surgical societies across the world have produced designated guidelines and recommendations to cope with the impact of the pandemic. Anticipated shortages of intensive care beds and medical personnel have been noted as a potentially critical issue for patients in need of emergent surgeries for acute abdominal issues and for oncologic safety. Guidelines announced at the start of the pandemic were largely focused on treating emergent patients and updates were published to reflect the accumulated clinical data.
This review aimed to condense the vast clinical data that has been shared globally in order to accurately summarize the current surgical practices in the COVID-19 era, the influence that the pandemic has had on surgical outcomes, and the safety criteria issued by surgical societies to assist their members with the impacts of this pandemic.
METHODS
A literature search for eligible studies was undertaken in March 2022 using PubMed databases. Search keywords included “COVID” and “surgery” or “surgical.” Initial searches revealed more than 1.6 million published reports in both 2020 and 2021. There were a further 440,000 results in the first 3 months of 2022. From these voluminous search results, review articles reported in major journals related to general surgery were preferentially selected for a more detailed perusal. Abstracts were screened to identify multinational multicenter-based studies to be evaluated as a priority. Grey literature announced by health organizations based on national or global health authorities were identified from references in the included published research papers. All levels of evidence were included. All studies presenting clinical outcomes after surgery during the pandemic period were thoroughly reviewed.
RESULTS
Real world impacts of COVID-19 on surgical practice
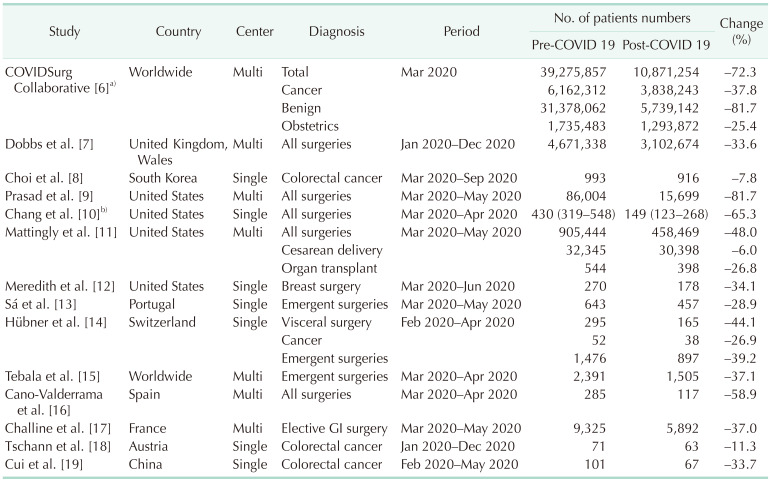
Throughout the course of the pandemic, many medical centers simultaneously reported a decrease in their numbers of surgeries, whether they were elective or emergent, or for cancerous or benign resections. The initial prediction made by the COVIDSurg Collaborative group was an 80% decrease in benign and a 30% decrease in malignant cancer surgeries (Table 1) [678910111213141516171819]. A multicenter-based report from England and Wales reported a 33.6% decrease in all types of surgeries in 2020 compared to non-pandemic periods (4,671,338 to 3,102,674) [7]. Similarly, elective surgery cases in the United States (US) showed a dramatic decrease (34.1% to 81.7%) in several reports, including 2 multicenter studies in the period from March to May 2020 compared to the same months in 2019 [9101112]. In addition to elective surgeries, emergent operations have also been reported to decrease by around 30% worldwide [131415]. Cancer surgeries and obstetric operations have been less affected with centers reporting only a 7.8% reduction in colorectal cancer resections [8] and a 6% drop in cesarean deliveries [11]. Notably, these decreases in the US recovered to nearly 2019 levels after healthcare systems adapted to the pandemic, even during the peak burden of the disease [911]. A national observational study conducted in England predicted that by the end of 2021, 2.4 million surgeries would be overdue [7]. A nearly 5 million surgical case backlog has been estimated in the US alone, and it is clear that dealing with this will be an arduous task [20].
Short-term postoperative outcomes: elective operations
Guidelines from various surgical societies issued in March 2020 mostly recommended postponing elective surgeries indefinitely and focusing on emergency operations. Reducing elective operations had benefits in releasing general ward and intensive care unit beds to treat COVID-19 patients. Also, there was no information on outcomes after surgery during the pandemic at that time [21]. At present, however, centers around the world have been reporting the clinical outcomes of elective operations during the pandemic period.
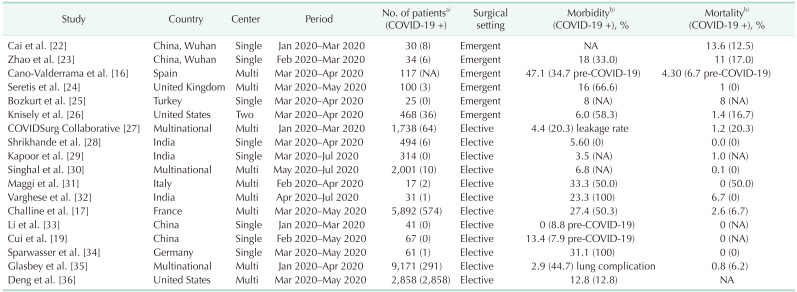
Twelve studies were reviewed for elective surgery outcomes during the COVID-19 pandemic (Table 2) [161719222324252627282930313233343536]. All of these reports presented postoperative morbidity and mortality data that were comparable to the pre-pandemic era. The average leakage rate after colorectal cancer surgeries was 4.9% and the mortality rate was 1.8%. Postoperative COVID-19 infection was significantly associated with mortality (adjusted odds ratio, 16.90; P < 0.001), which required surgeons to undertake stringent mitigation measures [27]. Furthermore, the leakage rate presented in this study was comparable to those of around 10% reported in the pre-pandemic era [3738]. In addition, a further study reported a 10-fold increase in mortality among symptomatic COVID-19 patients but only a 2-fold increase in asymptomatic patients after gastrointestinal surgery. Systematic screening for the virus has therefore been recommended before conducting elective surgeries [17].
A recent retrospective study in the US has presented the results of major elective surgeries in patients infected with COVID-19. Surgery within 0 to 4 weeks of a positive COVID-19 test was found to be significantly associated with pulmonary complications, while patients who underwent surgery more than 8 weeks after a COVID-19 infection did not show any increased morbidity [36]. Other studies have presented similar results, thus recommending that COVID-19 positive patients not undergo any surgery until at least 7 to 8 weeks have passed [3940].
Short-term postoperative outcomes: emergent operations
In spite of the higher risk of postoperative morbidity (especially pulmonary complications) in COVID-19 patients, and the possibility of spreading the virus during hospitalization and surgery, there are always going to be situations where an immediate surgical intervention has to be performed to save the life of the patient. From the start of the pandemic in March 2020, many studies have repeatedly insisted that surgeons should not hesitate to perform urgent operations when necessary. Six studies were reviewed regarding surgical outcomes after urgent operations during the COVID-19 era (Table 2) [162223242526]. These reports included positive COVID-19 cases. Although COVID-19 again showed a significant association with postoperative morbidity and mortality [26], the majority of noninfected patients could be treated successfully with stringent mitigation protocols in place, and the outcomes, including adverse events, were comparable to those found in the pre-pandemic period [41]. The postoperative COVID-19 infection rate was reported to be around 3% [24].
Concerns regarding malignant disease
Tumor progression can occur in as little as 4 to 8 weeks in certain cases and delaying surgery in colorectal cancer by more than 30 to 40 days is reported to be associated with poorer overall survival in several studies [424344]. A prior systemic review and meta-analysis had recommended that colorectal cancer surgery should not be postponed for longer than 4 weeks [45]. The tumor volume doubling time of a primary lesion is dependent on the type of cancer and its organ of origin but delaying a resection procedure by more than 30 days is generally reported to be unfavorable [464748].
As noted in an earlier section, the backlog of surgeries due to COVID-19 in England now represents more than 6 months of pre-pandemic surgical procedures [7]. It has also been predicted that it will require up to 3 months to clear the current backlog of overdue surgeries in the US alone [20]. Hence, restoring surgical capacities to pre-pandemic levels is important and revisions to current clinical practices should be considered to achieve this, if feasible. The American College of Surgeons guidelines for elective cases recommend considering neoadjuvant chemotherapy for 2 to 3 months in colon cancer patients in the COVID-19 era [49]. Also, the Society of Surgical Oncology recommends neoadjuvant therapy for resectable pancreatic cancer and selected gastric cancer cases as a temporary measure during the pandemic [50]. Although resection of primary cancer is the treatment of choice for most gastrointestinal malignancies, advances in adjuvant treatments have provided clinicians with alternative measures to cope with the current circumstances [515253].
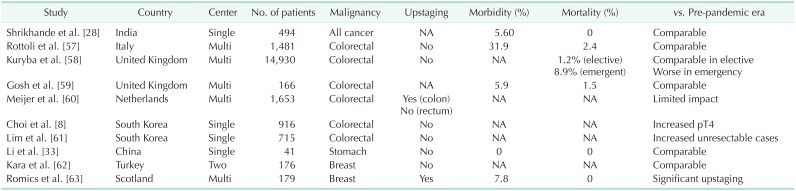
Some reports have indicated that cancer patients are more vulnerable to the severe complications associated with COVID-19 [5455]. Despite this, the continuance of cancer treatment is recommended by the Korean Cancer Association [56]. Clinicians must treat cancer patients in accordance with their individual characteristics, the involved organ(s), the tumor stage, and the available adjuvant treatments. Although some studies have indicated an increase in T4 stage cancer during the pandemic, most have reported no significant upstaging in terms of the TNM classification (Table 3) [8283357585960616263]. A hasty or obstinate selection of surgical resection is thus unnecessary in positive COVID-19 cases if other treatment modalities are available. Furthermore, the use of telehealth or telemedicine applications, in which clinicians assess and manage patients without direct contact, has also emerged and been adopted rapidly as a countermeasure [51646566].
Choice of surgical modality
Virus transmission during the pandemic has been one of the prime concerns for surgeons. Airborne spread may occur not only during intubation and extubation but also during the procedures when fumes are created by surgical devices [67]. Early in the COVID-19 era, a study proposed that although there was insufficient evidence to prove that minimally invasive surgery (MIS) was safe in terms of transmission, this method could be performed while adhering to necessary precautions. Recommendations from the United Kingdom and Ireland Intercollegiate Board, however, were that MIS was generally not to be used during the pandemic and that laparoscopy should be considered only in selected individual cases [68].
After 2 years of surgical experiences during the COVID19 pandemic, a number of studies have reported that MIS is safe and feasible. A study in England revealed no difference between MIS and open surgery regarding the transmission rate to 14 staff members during 73 operations [69]. A Japanese group quantified the particulate matter counts in surgical smoke from both laparoscopic and open surgery in colorectal disease. The results showed lower exposure to surgical smoke during laparoscopic surgery compared to open surgery [70]. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) summarized studies on MIS during the pandemic era and reported its results recently. A case report did not detect viral particles in the surgical fume directly taken from the trocar [71], and a case series detected SARS-CoV-2 in the surgical plume but no medical staff member was infected due to the exposure [72]. SAGES summarized MIS to be safe and concluded that either MIS or an open approach can be performed in COVID-19 patients [73].
Updated guidelines from different medical societies
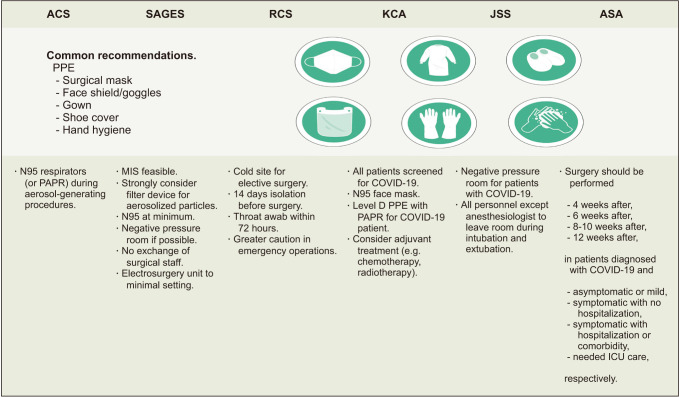
Numerous sets of guidelines have now been produced from medical societies around the world since the beginning of the COVID19 pandemic. There are slight distinctions between them as they aim to optimize procedures in accordance with the requirements of each nation’s population (Fig. 2) [6874757677]. Overall, the backbone of most sets of guidelines is based on WHO and Centers for Disease Control and Prevention recommendations, which are also supported by evidence from various reports. The interim guidance announced by WHO in June 2020 recommended molecular assays of upper respiratory specimens from any patient showing signs or symptoms of COVID-19. This can be modified depending on local testing capacity and testing should also be conducted on all patients before a surgical procedure regardless of the risk assessment for COVID-19. Staff participating in surgical procedures for a COVID-19 patient should use sterile medical mask, face shield or goggles, gloves, and gown. An N95 mask should be used when aerosol-generating procedures are being conducted. A negative pressure room would be ideal in these instances if available [78]. Dedicated operating theatres for COVID-19 patients are also recommended but can be used for negative patients after terminal cleaning. The number of surgical staff in the theatre should also be limited to essential personnel only [79]. Patients should be isolated for at least 14 days if they have had contact with COVID-19 patients prior to surgery [80]. The Korean Cancer Association suggests that all patients be screened for COVID-19 prior to surgery and that personal protective equipment (PPE) for surgical staff should include double gloves, N95 masks, face shields or goggles, surgical caps, surgical gowns, and surgical shoe covers for all procedures. Level D PPE powered using an air-purifying respirator (powered air-purifying respirator [PAPR]) is also recommended for performing surgery on COVID-19 patients [59]. Recommendations from selected international societies are summarized in Fig. 2.
CONCLUSIONS
The challenges facing surgical teams during the COVID-19 pandemic remain ongoing. Guidelines were mostly enacted shortly after the pandemic was officially announced and are being continually updated in accordance with its progression. However, COVID-19 is showing a peak surge at the time of writing compared to the past 2 years and the existing guidelines are not based on the most severe recent rise in COVID-19 patients. Predictions of the pandemic’s course have now been widely exceeded and it would also be a conjecture to consider that the current situation could not worsen further.
It must be noted, however, that performing essential surgeries for patients in need has proven to be feasible during this health crisis. Adherence to the basic precautions from global health organizations and to any modified recommendations from local surgical organizations has been found to be practicable, as reported by various studies from different regions of the world. It is crucial, that health care systems and surgical staff remain vigilant and attentive to the ever-changing situation in this pandemic in order to provide optimal medical support to their patients.
There were several limitations to this present review of note. Although articles related to surgical safety in the COVID-19 era were searched as thoroughly as possible, it was obviously not possible to review all of the more than 3 million papers published to date and some information could have been overlooked. Also, as previously discussed, the data from the included studies in our present review do not reflect the current situation in the pandemic or the progression of the COVID-19 virus.
 XML Download
XML Download