

 PDF
PDF Citation
Citation Print
Print



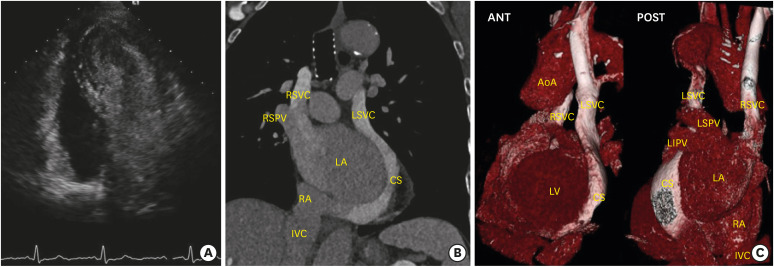
An eighty-three years-old female with a history of multiple idiopathic strokes was referred to our hospital with stroke relapse. We performed a transthoracic echocardiogram that underlined a dilated coronary sinus (CS) despite the absence of a cause for elevated right atrial pressure. Through agitated saline (AS) injection in a left antecubital vein, a persistent left superior vena cava (LSVC) was identified by the classical appearance of microbubble earlier in the CS than in the right atrium (RA). As part of our protocol, we also injected AS in a right antecubital vein, and interestingly, the microbubble filled only the left cavities, demonstrating a right-to-left shunt (RLS) (Figure 1A and Supplementary Video 1). Computed tomography scan showed, along with the persistent LSVC, an anomalous right superior vena cava (RSVC) complete drainage into the left atrium (LA) (Figure 1B and C). This cause of RLS is extremely rare in association with a persistent LSVC and could explain the patient's multiple stroke history. At the heart team evaluation, a conservative approach was recommended because of the patient's age and comorbidities, and oral anticoagulation was initiated.
In conclusion, the anomalous RSVC drainage was suspected, in addition to the persistent LSVC, thanks to the AS injection also in the right arm, underscoring the importance of routinely performing echocardiographic bubble study through both sides. Written informed consent was obtained from the patient in Figure 1.

 XML Download
XML Download