

 PDF
PDF Citation
Citation Print
Print



An 89-year-old woman underwent transfemoral transcatheter aortic valve replacement with a 26-mm Evolut PRO (Medtronic, Minneapolis, MN, USA) bioprosthesis because of severe aortic stenosis.
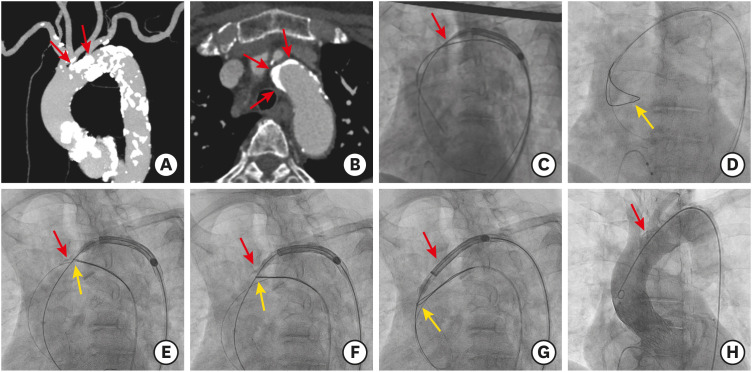
As shown in Figure 1, the delivery catheter failed to pass through the severely calcified aortic arch, because of a dense calcified mass in the outer curvature of the aortic arch (Supplementary Video 1). Eventually, a snare-assisted delivery using a 35-mm loop Amplatz Goose Neck Snare kit (ev3 Endovascular, Inc., Plymouth, MN, USA) was attempted. We tightened the snare to grasp and retain the stiff wire and the nose cone of the delivery catheter. Further, we advanced the delivery catheter while simultaneously pulling the snare catheter downward. Finally, the delivery catheter was passed and the valve implantation was successful without major aortic complications (Supplementary Videos 2 and 3).
Severely calcified aortic arches are a major limitation in the implantation of currently available self-expanding valves due to the rigidity and non-steerable features of these valves, with the risk of delivery failure or fatal complications including aortic dissection or rupture.1) The inflexible and bulky delivery catheter tends to follow the outer curvature of the aortic arch, and massive calcification can obstruct the device passage. The snare technique can direct the wire and delivery catheter away from the aortic wall, leading to successful crossing.
In an extremely calcified aortic valve and a horizontal aorta that blocks the passage of a bioprosthetic valve, a snare catheter can achieve coaxiality with the aortic orifice and successful crossing of the aortic valve.2)

 XML Download
XML Download