

 PDF
PDF Citation
Citation Print
Print


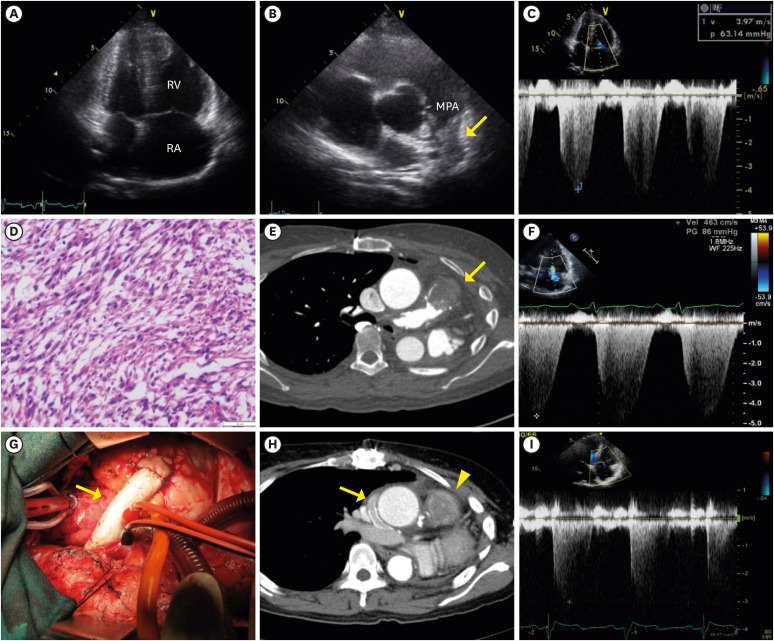
A 47-year-old female presented with progressive dyspnea for 1 year. Transthoracic echocardiography showed enlargement of right atrium and right ventricle (RV, Figure 1A), a mass in the main pulmonary artery (MPA, Figure 1B), and elevated right ventricular systolic pressure (RVSP, 94 mmHg, Figure 1C). The patient underwent left pneumonectomy and graft replacement of the MPA along with the proximal left and right pulmonary arteries. Pathology revealed grade 2 pulmonary artery leiomyosarcoma (Figure 1D). After adjuvant chemotherapy, there was no evidence of tumor recurrence. However, aggravating dyspnea recurred at 7 years after surgery. On computed tomography (CT, Figure 1E), tumor was found at the junction of the RV and MPA. Moreover, there was markedly elevated RVSP (101 mmHg, Figure 1F). Because complete surgical resection was impossible due to wide extension of the tumor, a 16 mm Gore-tex conduit was installed between the RV and the right pulmonary artery (Figure 1G). After the bypass surgery, patent bypass conduit was confirmed on CT (Figure 1H) and the previously elevated RVSP decreased to 36 mmHg (Figure 1I). After post-radiotherapy, the patient did not present any symptoms implying pulmonary hypertension and there was no evidence of disease progression on follow-up images for 6 years. Although the median survival time of pulmonary artery leiomyosarcoma is 10 months, she has survived more than 13 years since initial diagnosis due to aggressive multimodal treatment. As shown in this case, palliative surgery with radiotherapy can be beneficial for long-term survival of patients with recurrent pulmonary artery leiomyosarcoma.
Dong Seon Kang, MD , Hee Jun Park, BS, Chi Young Shim, MD, PhD, Geu Ru Hong, MD, PhD, Jiwon Seo, MD
, Hee Jun Park, BS, Chi Young Shim, MD, PhD, Geu Ru Hong, MD, PhD, Jiwon Seo, MD
, Hee Jun Park, BS, Chi Young Shim, MD, PhD, Geu Ru Hong, MD, PhD, Jiwon Seo, MD
Figure 1
Various images obtained during long-term treatment. (A) Markedly enlarged right atrium and ventricle were observed on TTE. (B) A supra-valvular mass-like lesion was seen in MPA (yellow arrow). (C) Markedly elevated RVSP (94 mmHg) caused by the obstructive mass lesion. (D) Pathologic study showed grade 2 pulmonary artery leiomyosarcoma, characterized as a well-demarcated mass composed of fascicular growth and an 11/10 high power field mitotic count. (E) Chest CT scan reveals a 3 cm recurred leiomyosarcoma (yellow arrow) at the junction area between the RV and MPA. (F) Markedly elevated RVSP (100 mmHg) was observed. (G) A 16 mm Gore-tex conduit (yellow arrow) insertion between RV and right pulmonary artery was performed to relieve severe right ventricular pressure elevation. (H) Post-operative chest CT scan showed that right pulmonary artery was well enhanced by contrast through a patent Gore-tex conduit (yellow arrow). A remnant leiomyosarcoma at proximal MPA was seen (yellow arrowhead). (I) Decreased RVSP (36 mmHg) was observed on TTE after successful bypass surgery.
CT = computed tomography; MPA = main pulmonary artery; RV = right ventricle; RVSP = right ventricular systolic pressure; TTE = transthoracic echocardiography.
 XML Download
XML Download