

 PDF
PDF Citation
Citation Print
Print



A 66-year-old male patient presented to the emergency room with progressive dyspnea and fatigue for one month. He had a history of bioprosthetic aortic valve replacement and separated graft implantation to the ascending aorta 5 years ago. Three months after surgery, he had infective endocarditis due to staphylococcus epidermidis. At end of 6 weeks of antibiotic treatment, the total cure for endocarditis was achieved.
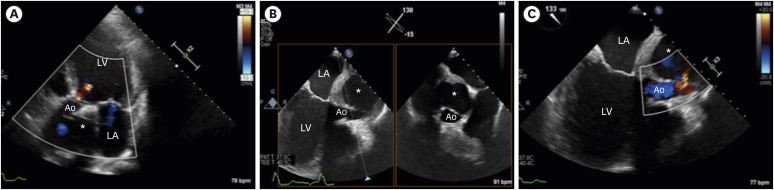
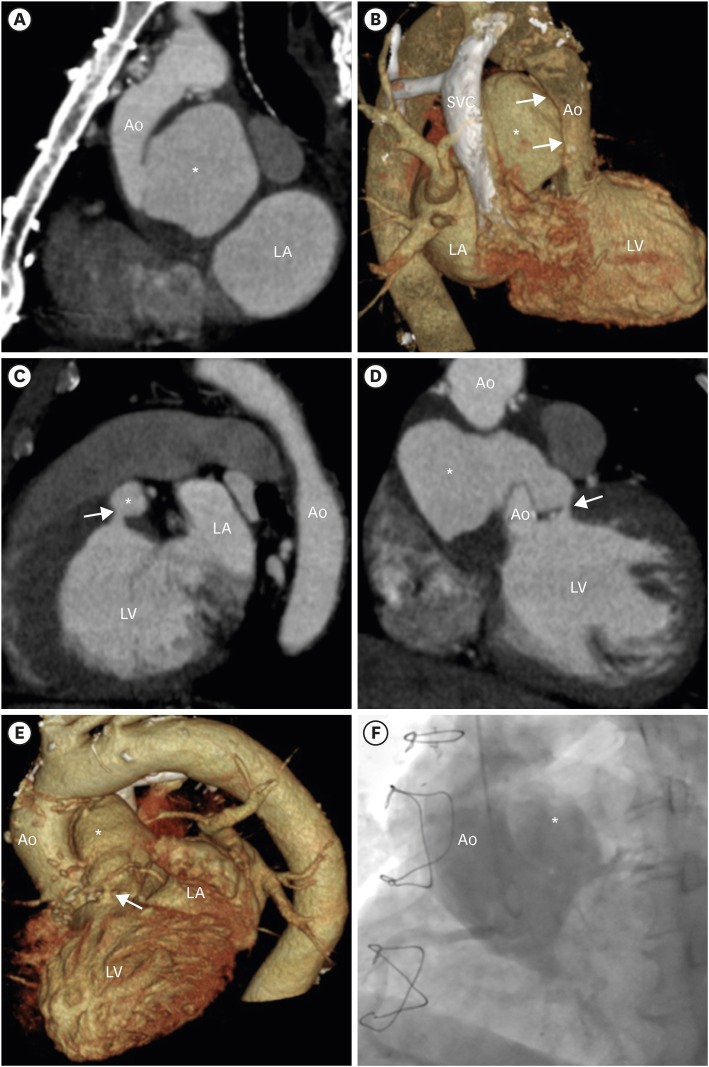
After five years, diminished left ventricular (LV) systolic function was detected in transthoracic echocardiography (TTE), which was normal before, and LV ejection fraction was measured as 25%. The pseudoaneurysm of the aortic graft was detected in TTE (Figure 1A, Supplementary Video 1). In transesophageal echocardiography (TEE) examination, severe compression of aortic graft by the pseudoaneurysm was shown (Figure 1B, Supplementary Video 2). Flow from graft into the pseudoaneurysm was present during both systole and diastole (Figure 1C, Supplementary Video 3). For further evaluation, computed tomographic angiography (CTA) was performed. Pseudoaneurysm of the aortic graft was also demonstrated by CTA. Severe compression to aortic graft was observed (Figure 2A and B). Also, there was a fistulization from the pseudoaneurysm into the left ventricle which we could not detect in echocardiography (Figure 2C-E). The lumen of the pseudoaneurysm was communicated with aortic graft and left ventricle both and this co-occurrence caused abnormal shunt from the aorta to the left ventricle which is similar to aortic valve regurgitation hemodynamically. Diastolic flow to pseudoaneurysm suggests that there is a flow from aortic graft to the left ventricle through the fistula (Supplementary Video 3). Aortography was performed and filling of contrast from the aorta to the pseudoaneurysm was observed (Figure 2F, Supplementary Video 4). Surgery was recommended to the patient but he refused the treatment.
 XML Download
XML Download