

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Previous randomized controlled trials (RCT) showed significant angina relief and quality of life improvement after percutaneous coronary intervention (PCI) compared with optimal medical therapy (OMT) alone. Despite various methods to assess the effect of PCI on symptom improvement,1) the subjective nature of angina relief provoked the need for a more objective measure of improvement to assess the efficacy of PCI. In this regard, some studies evaluated exercise capacity, which is also a strong prognostic factor,2)3) to compare the efficacy of PCI with OMT.4)5)6)
Although an earlier trial reported a significant increase in exercise duration in patients who underwent PCI,4) later trials, including the most recent Objective Randomized Blinded Investigation with optimal medical Therapy of Angioplasty in stable angina (ORBITA) trial, showed unclear benefit of PCI in increasing exercise duration compared with OMT plus placebo procedure.5)6) It should be noted that previous studies only included patients with single vessel disease which could limit the baseline extent of myocardial ischemia and had a relatively short follow-up period which might not reflect the benefit of revascularization that is known to be extended to 24 months after the procedure.1)
Therefore, we sought to compare the changes in exercise duration and long-term clinical outcomes according to the relief of myocardial ischemia by comparing pre- and post-PCI exercise stress test (EST) results.
METHODS
Study population
Between January 2003 and June 2011, PCI was performed in 5,929 patients at Samsung Medical Center. A total of 3,208 patients underwent elective PCI for stable ischemic heart disease (SIHD). After excluding patients with coronary computed tomography alone or no stress testing, or those with pharmacologic stress echocardiography of nuclear study prior to PCI, 959 patients who had EST within 6 months prior to PCI were selected. For study purposes, the 291 patients who did not have a positive result of pre-PCI EST (173 patients with suboptimal heart rate and 118 patients with ST depression less than 1 mm) were excluded. Among the remaining 668 patients, 396 patients who did not undergo follow-up EST within 24 months after PCI, 2 patients who underwent EST by modified Bruce protocol, and 14 patients who had nonfatal myocardial infarction (MI) or any revascularization before follow-up EST (Supplementary Figure 1) were excluded. Post-PCI EST was performed as routine follow-up protocol of the patients under institutional policy. Finally, a total of 256 eligible patients were divided into 2 groups according to the functional completeness of revascularization: 1) the functional complete revascularization (CR) group had positive EST before PCI and negative EST after PCI (n=149); and 2) the functional incomplete revascularization (IR) group had positive EST both before and after PCI (n=107).
Patient follow-up
Clinical, angiographic and procedural data were recorded prospectively by independent research personnel. Patients were routinely followed up at 1, 6, and 12 months after index procedure and annually thereafter. Further information was collected by telephone contact and medical records if necessary. Follow-up was considered complete if the patient's death was confirmed by the National Population Registry of the Korea National Statistical Office using a unique personal identification number, or if the patient was contacted at the planned follow-up interval. The Institutional Review Board and Ethics Committee approved this study and waived the requirement for written informed consent for access to an institutional PCI registry (2016-03-020).
Coronary angiography analysis
Angiographic disease severity was assessed by Synergy Between PCI With Taxus and Cardiac Surgery (SYNTAX) score and residual disease burden after PCI was assessed by residual SYNTAX score in an independent core laboratory by a blinded investigator. In patients with functional IR, post-PCI coronary angiograms were reviewed by 2 independent investigators to explore potential reasons for positive post-PCI EST results.
Exercise stress test
The EST was performed according to the Bruce protocol using a conventional treadmill. A 12-lead electrocardiogram (ECG) was recorded and monitored continuously with a computerized system (Quinton Q-Stress; Quinton Cardiology, Inc. Bothell, WA, USA) during exercise and rest. The ECG was reviewed by cardiology fellows and senior cardiologists. The test was discontinued in the event of exercise-limiting symptoms including dyspnea, chest pain, fatigue, or significant abnormalities in vital signs. The target heart rate was determined as 85% of maximum predicted heart rate (220 − age), but was not used as a predetermined endpoint for premature termination of the test. A positive result was defined as horizontal or down-sloping ST depression ≥1 mm (0.1 mV) at 60 to 80 milliseconds after the J point,7) by using the largest value of ST-deviation during exercise or recovery phase. In patients with baseline ECG abnormalities, 3 or more consecutive beats in the same lead with a stable ECG baseline were analyzed. In case of unstable baseline, an average magnitude of consecutive beats was analyzed, and if required, computer-assisted ECG were included in analysis. In patients with baseline ST segment change, an additional ST depression from baseline level was analyzed. In patients with resting ST segment elevation, a magnitude of ST depression below baseline PQ segment was used for interpretation. The Duke score was calculated as follows: duration of exercise in minutes − (5 × the maximal ST-segment deviation from baseline during or after exercise, in millimeters) − (4 × angina index). The angina index was defined as 0 if the patient had no angina during exercise, 1 if the patient had non-limiting angina, and 2 if angina was the reason for the patient stopping the exercise.8) Duke treadmill score was calculated regardless of EST result for comparison.
Out of 256 patients, 27 patients who showed definite ST segment depression in pre-PCI EST did not reach target heart rate without ST depression on post-PCI EST during their maximal exercise. Those patients were considered as having negative EST.
Study outcomes
The primary outcome was change in exercise duration after PCI and was calculated as the difference in exercise duration between pre-PCI and post-PCI ESTs. Secondary outcomes were major adverse cardiac events (MACE, a composite of all-cause death, any spontaneous MI, and any ischemia-driven revascularization) and individual components of MACE at 3 years of follow-up. Spontaneous MI was defined as elevated cardiac enzyme levels, such as troponin I or myocardial band fraction of creatine kinase, greater than the upper limit of the normal range with either ischemic symptoms or electrocardiographic changes indicating ischemia after index procedure.9) Periprocedural MI was not included as a clinical event. Ischemia-driven revascularization included all target and non-target revascularization with either PCI or coronary artery bypass graft surgery. Ischemia-driven revascularization was defined as a revascularization procedure with at least one of the following: 1) Recurrence of angina; 2) Positive non-invasive test other than EST; and 3) Positive invasive physiologic test.
Statistical analysis
Continuous variables were presented as mean±standard deviation or median (Q1–Q3) according to the normal distribution. To compare differences of variables between groups, Student's t-test or the Mann-Whitney U test was used for continuous variables, and χ2 test was used for categorical variables. To compare continuous variables between pre-PCI and post-PCI EST within the same group, paired t-test was used. To determine the significance of relationship between exercise duration increment and post-PCI EST result, multivariable linear regression was performed using clinically relevant variables including age, sex, hypertension, diabetes, previous PCI, previous MI, baseline (pre-PCI) exercise duration, and days from PCI to post-PCI EST. Linear regression analysis was used to evaluate the association of a change in exercise duration with pre-PCI Duke treadmill score or pre-PCI SYNTAX score.
As a sensitivity analysis, a propensity score-adjusted multivariable regression was performed for comparison of exercise increment between the 2 groups. Propensity score was estimated by multivariable logistic regression analysis using all baseline clinical characteristics and disease extent. Estimated propensity score was added to the multivariable adjusted variables.
Event rates were calculated based on Kaplan-Meier censoring estimates and presented with the cumulative incidence, and the log-rank test was used to compare survival curves between groups. Multivariate Cox proportional hazard regression was used to calculate adjusted hazard ratio (HRadj) and 95% confidence interval (CI) to compare between-group differences. In multivariate linear regression and multivariate Cox proportional hazard model, clinically relevant variables including age, sex, hypertension, diabetes mellitus, previous PCI and previous MI were included. The assumption of proportionality was assessed graphically by the log-minus-log plot, and Cox proportional hazard models for all clinical outcomes satisfied the proportional hazards assumption.
All probability values are 2-sided and p values <0.05 were considered statistically significant. R software version 3.4.0 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses.
RESULTS
Patient characteristics
A total of 256 patients eligible for analysis met the following inclusion criteria: 1) positive result of pre-PCI EST; 2) elective PCI for SIHD; 3) available post-PCI EST results; and 4) no clinical event of MI or any revascularization before post-PCI EST (Supplementary Figure 1). Among the total population, 149 patients were classified as the functional CR group based on negative conversion of post-PCI EST whereas 107 patients were classified as the functional IR group based on remaining positive results in post-PCI EST. Baseline characteristics were not significantly different between the 2 groups, except higher prevalence of hypertension and previous PCI in the functional IR group (Tables 1 and 2). Both groups showed minimal residual stenosis after PCI with similar residual SYNTAX score. Among patients with functional IR, potential reasons for positive post-PCI EST results were suspected due to residual focal stenosis with angiographic %DS≥50% including chronic total occlusion and compromised side branch (25.2%), suspected diffuse atherosclerosis in angiography without focal stenosis (67.3%), and unknown or suspected combined microvascular disease (7.5%).
Table 1
Baseline clinical characteristics
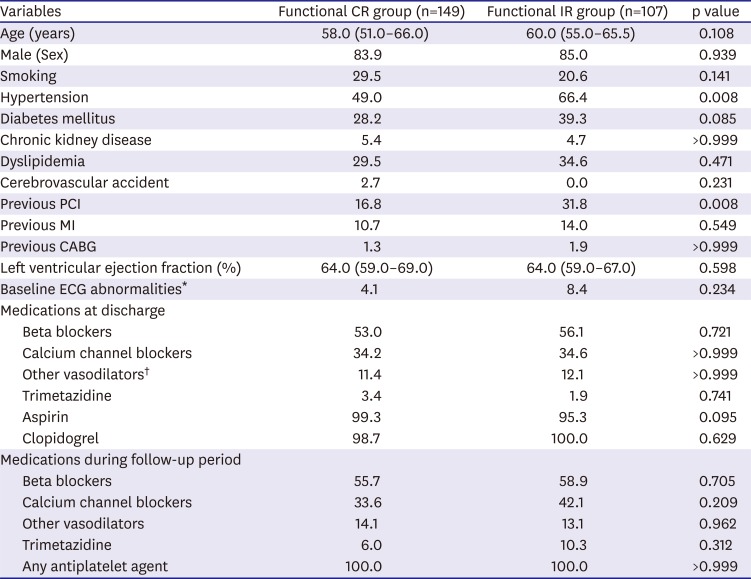
Values are presented as mean±standard deviation or median (Q1–Q3) or percentage as appropriate.
CABG = coronary artery bypass grafting; CR = complete revascularization; ECG = electrocardiogram; IR = incomplete revascularization; MI = myocardial infarction; PCI = percutaneous coronary intervention.
*Atrial fibrillation left ventricular hypertrophy, ST/T segment changes, and bundle branch block; †Nicorandil, isosorbide mononitrate, isosorbide dinitrate, and molsidomine.
Table 2
Angiographic and procedural characteristics
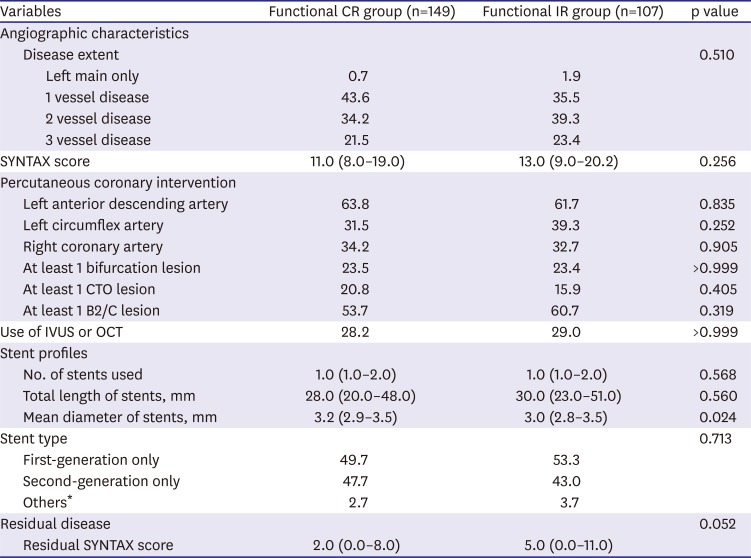
Values are presented as mean±standard deviation or median (Q1–Q3) or percentage as appropriate.
CR = complete revascularization; CTO = chronic total occlusion; IR = incomplete revascularization; IVUS = intravascular ultrasound; OCT = optical coherence tomography; SYNTAX = Synergy between PCI with Taxus and Cardiac Surgery.
*Others included simultaneous use of bare metal, first-generation, or second-generation stents.
Pre-percutaneous coronary intervention exercise stress test between the 2 groups
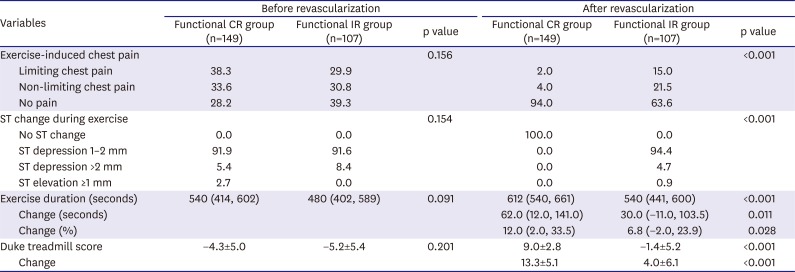
Details of EST are shown in Table 3. In pre-PCI EST, about 60% of patients in both functional CR and IR groups showed exercise-limiting or non-limiting chest pain during EST without between-group difference. The median exercise duration before PCI was similar between the functional CR and IR groups (540 [Q1–Q3, 414, 602] seconds vs. 480 [Q1–Q3, 402, 589] seconds, p=0.091). Pre-PCI Duke treadmill score represented that the study population was moderate-risk population, and there was no signfiicant difference between the 2 groups.
Table 3
Results of exercise stress testing before and after revascularization
Post-percutaneous coronary intervention exercise stress test and changes of exercise duration between the 2 groups
The median time interval of post-PCI EST after the index procedure was 269 days (Q1–Q3, 166, 393) with median 10 days difference between the 2 groups (median 274 vs. 264 days for functional CR and IR group, respectively, p=0.012). After PCI, the functional CR group had significantly greater relief of exercise-induced chest pain and less incidence of significant ST-segment change during exercise. Median exercise duration was significantly higher in the funtional CR group than in the functional IR group (612 [Q1–Q3, 540, 661] seconds versus 540 [Q1–Q3, 441, 600] seconds, p<0.001). In addition, the Duke treadmill score was also significantly higher in the functional CR group than in the functional IR group.
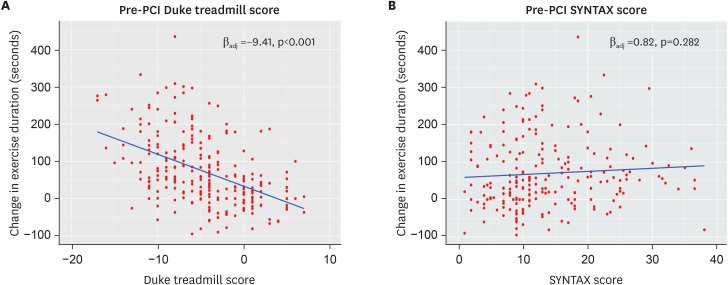
When the amount of change in exercise duration and Duke treadmill score was compared between the 2 groups, the functional CR group showed a significantly higher increment in exercise duration (62.0 [Q1–Q3, 12.0, 141.0] seconds vs. 30.0 [Q1–Q3, −11.0, 103.5] seconds, p=0.011) as well as Duke treadmill score (Figure 1). The increment in exercise duration was also significantly different after adjustment of baseline covariables between the functional CR and IR groups (βadj=40.1 seconds, p<0.001), and the consistent result was observed in sensitivity analysis (βadj=44.4 seconds, p<0.001). The increment of exercise duration had a significant inverse relationship with pre-PCI Duke treadmill score (p<0.001). However, there was no significant relationship between the increment of exercise duration and pre-PCI SYNTAX score (p=0.282) (Figure 2).
Figure 1
Exercise duration according to functional completeness of revascularization. (A) Exercise duration before PCI; (B) Exercise duration after PCI; (C) Changes in exercise duration after PCI.
CR = complete revascularization; IR = incomplete revascularization; PCI = percutaneous coronary intervention.
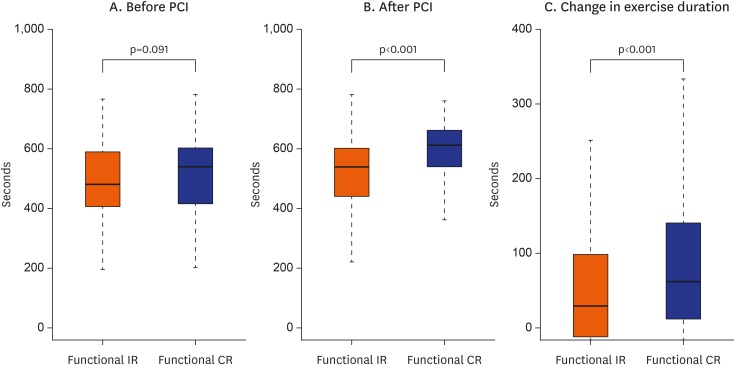
Figure 2
Changes of exercise duration after PCI according to pre-PCI functional and anatomical severity. (A) Pre-PCI Duke treadmill score and changes of exercise duration; (B) Pre-PCI SYNTAX score and changes in exercise duration. Correlation coefficient (beta) was adjusted for age, sex, hypertension, diabetes mellitus, previous percutaneous coronary intervention and previous myocardial infarction.
PCI = percutaneous coronary intervention; SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery.
Clinical outcomes at 3-years after percutaneous coronary intervention
The functional CR group showed a significantly lower risk of MACE (6.2% vs. 26.1%; HRadj, 0.18; 95% CI, 0.08–0.40; p<0.001), mainly driven by a significantly lower incidence of ischemia-driven revascularization than the functional IR group (Figure 3 and Table 4). The cause of ischemia-driven revascularization was due to refractory chest pain despite OMT with objective signs of lesion progression in 92.3% (24/26 events) of patients in the functional IR group and in 71.4% (5/7 events) of patients in the functional CR group.
Figure 3
Comparison of risk of major adverse cardiac events at 3 years. Hazard ratio and its p value were adjusted for age, sex, hypertension, diabetes mellitus, previous percutaneous coronary intervention and previous myocardial infarction.
CI = confidence interval; CR = complete revascularization; HRadj = adjusted hazard ratio; IR = incomplete revascularization.
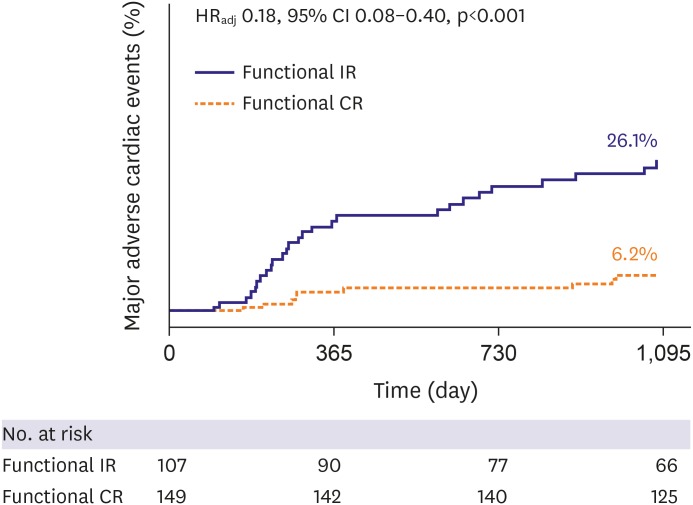
Table 4
Clinical outcomes at 3 years after revascularization

Values are number (%) or HR (95% confidential interval).
CR = complete revascularization; HR = hazard ratio; IR = incomplete revascularization; MI = myocardial infarction.
*Adjusted HR was calculated by multivariate Cox regression analyses with age, sex, hypertension, diabetes mellitus, previous percutaneous coronary intervention and previous MI.
DISCUSSION
The main findings of current study were as follows. First, the study population underwent PCI for SIHD with proven evidence of inducible myocardial ischemia by positive pre-PCI EST results and were considered as moderate-risk population by Duke treadmill score. Second, despite similar pre-PCI exercise duration and angina severity, those with negative conversion of post-PCI EST (funtional CR group) showed a significantly higher increment of exercise duration and lower angina severity than those with still positive post-PCI EST results (functional IR group). Third, the degree of exercise increment after PCI was significantly associated with pre-PCI functional severity, which was determined by the Duke treadmill score, but not with pre-PCI anatomical severity, which was determined by the SYNTAX score. Fourth, the functional CR group showed a lower risk of MACE at 3 years, mainly driven by a lower incidence of ischemia-driven revacularization, compared with the functional IR group.
Based on previous evidence which presented the lack of benefit in reducing death or MI by PCI in SIHD patients, symptom control has been a target treatment goal of PCI. When evaluating the efficacy of PCI on subjective symptoms, results are inevitably affected by placebo effect or various bias from self-reporting methods.10) Exercise capacity is an alternative parameter strengthened by being an objective and reproducible index, and is known to be a strong prognostic indicator in patients with coronary artery disease.11) Although there have been few RCTs evaluating exercise capacity after PCI, the results are heterogenous. In an earlier study, revascularization showed a higher increase of exercise duration by treadmill test than OMT.4) On the contrary, PCI was not found superior for increasing exercise duration compared with OMT in other studies, including the recent ORBITA trial.5)6)
However, previous study results had limited generalizability since patients with only single vessel disease was included. Degree of myocardial ischemia is a key factor related to prognosis of patients with coronary artery disease.12) Previous studies have shown that the benefit of revascularization in reducing myocardial ischemic burden was greater for patients with higher ischemic burden13) and revascularization also showed a higher prognostic impact over OMT in patients with moderate to large myocardial ischemic burden.14) The current study included patients with various severity of angiographic disease, a higher proportion of multivessel disease than previous studies, and higher risk profile represented by much lower Duke treadmill score than that of ORBITA trial.6)
Since angiographic severity is not concordant with functional severity,15) ischemia-directed revascularization based on non-invasive or invasive functional test is essential. Although EST does not determine the specific location of inducible myocardial ischemia related to the epicardial coronary stenosis, it can determine the patient-level existence of myocardial ischemia based on individual physical loads. In the present study, patients without remaining myocardial ischemia after PCI (functional CR) showed a higher increment of exercise duration as well as less exercise-induced chest pain than those with remaining myocardial ischemia (functional IR).
Myocardial ischemia affects exercise capacity through several possible mechanisms. First, exercise capacity is closely related with diastolic function during exercise, which has been known to be decreased by inducible myocardial ischemia.16) Second, previous studies presented reduced oxygen uptake kinetics and an inverse correlation between the severity of myocardial ischemia and oxygen uptake parameters, such as anaerobic threshold or time to O2 pulse flattening in patients with inducible myocardial ischemia.17)18) Third, exercise capacity could be limited by exercise-induced chest pain per se. Therefore, it seems reasonable that relieving myocardial ischemia would improve exercise capacity of patients with documented myocardial ischemia and the effect of revascularization might be greater in patients with higher myocardial ischemic burden or severity, which was also recently been supported by post-hoc analysis of the ORBITA trial.19) The findings that lower Duke treadmill score at baseline was significantly associated with higher exercise increment in our study, further support the association between the presence of patient-level myocardial ischemia and the benefit of PCI in increasing exercise duration.
Ischemia relief is also important to improve clinical outcome after PCI, and residual myocardial ischemia has been reported to be associated with worse prognosis.13)20) In the current study, patients with functional IR showed a higher rate of MACE at 3 years after index procedure, mainly driven by a higher incidence of ischemia-driven revascularization. The main reason of repeat revascularization was refractory chest pain despite OMT. Those results support the recently published final 5-year results of the FAME 2 trial, which presented significantly better clinical outcomes, including MI and urgent revascularization, after ischemia-directed revascularization than OMT alone.21) The current results are in line with the previous studies and underscore the importance of functional CR when revascularization is planned for patients with documented evidence of myocardial ischemia.
There are several limitations in the current study. First, it is a non-randomized observational study. Although baseline characteristics, including pre-PCI EST results, were similar between the 2 groups, unmeasured confounding variables might affect the results. Second, because post-PCI EST was performed based on operator discretion and exclusion of patients with clinical events before post-PCI EST, the possibility of selection bias should be considered. However, because routine use of post-PCI EST is not recommended by the appropriate use criteria,22) both groups showed comparable baseline characteristics and pre-PCI EST results, and the proportion of excluded patients due to clinical events before post-PCI EST was similar between the 2 groups, thus both groups might be comparable under similar chance of selection bias. Third, although the extent of residual disease was not significantly different between the functional CR and IR groups, detailed information on anatomical revascularization status after PCI was unavailable. Fourth, results of post-PCI ESTs could be affected by subclinical events which occurred before post-PCI EST. However, the median interval of post-PCI EST after index procedure was not much different from previous studies.4)5) Fifth, there might be possibility of interval progression of coronary artery disease before post-PCI EST. However, change of atheroma volume is generally minimal up to 24 months during medical threapy according to previous intravascular ultrasound studies.23)24) Last, the burden of myocardial ischemia assessed by non-invasive stress imaging tests could not be evaluated.
Following PCI in SIHD patients, those with functional CR showed a higher increment of exercise duration and lower risk of MACE than those with functional IR.
 XML Download
XML Download