

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common form of clinical arrhythmia associated with various cardiac and cerebrovascular events, and its prevalence is continuously increasing in societies with aging population.1) Patients are especially vulnerable in perioperative periods to such events resulting from factors such as hemodynamic changes, increased sympathetic tone, tendency for myocardial ischemia, surgery-induced stress, and cessation of anticoagulants.2)3) Despite the development in many aspects of perioperative management, reduction of major adverse cardiovascular and cerebrovascular event (MACCE) after noncardiac surgery has been modest at best.4) Therefore, better tools for defining the high-risk group for perioperative adverse events need to be developed.
AF is closely associated with the cardioembolic strokes which result in permanent neurologic deficits and mortality.5) Moreover, AF is also related to the overall postoperative cardiac and cerebrovascular events.6)7) However, AF itself is currently not included in routine perioperative risk assessments,8)9) and its overall impact on postoperative cardiac or cerebrovascular events remains unclear.10)11)12) We hypothesized that preoperative AF is an independent risk factor for perioperative cardiovascular event, and tested our hypothesis in a large-sized retrospective cohort that underwent both non-cardiac surgery and comprehensive preoperative cardiac evaluation.
METHODS
Study population
Of 327,216 patients who underwent surgery from November 2009 to March 2016 at Asan Medical Center in Seoul, Korea, we excluded patients who 1) underwent cardiac surgery (n=4,528); 2) did not undergo a comprehensive cardiac evaluation (n=295,982); or 3) has mitral stenosis or prosthetic valve (n=205). The main study population therefore comprised 26,501 (8.1%) patients who received comprehensive cardiac evaluation prior to undergoing non-cardiac surgery. This study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Review Board of Asan Medical Center (2018-1445), which waived the need for informed consent due to the retrospective nature of the study.
Data collection and definition of variables
The comprehensive cardiac evaluation for risk stratification included a 12-lead electrocardiogram (ECG), routine chest radiography, transthoracic echocardiography, and myocardial perfusion imaging (MPI). At our institution, patients scheduled for elective non-cardiac surgery were initially evaluated by the attending surgeon in the respective outpatient clinic or during hospitalization. The initial evaluation consisted of a dedicated investigation of the patient's medical history, comorbidities, and functional capacity. If the patient's functional capacity could not be measured or if relevant clinical risk factors for peri-operative cardiovascular outcomes existed, non-invasive testing was performed.8)9) By considering the expected cardiovascular risk, the attending surgeon made the decision to proceed with surgery, with consensus from cardiologists, neurologists, and anethesiologists.
ECGs were recorded at a gain of 10 mm/mV and paper speed of 25 mm/seconds. All ECGs were reviewed for AF by an independent cardiologist blinded to the outcomes. Patients were considered to have AF when AF was documented in any ECG taken before the index surgery. Persistent or permanent AF was defined as documented AF on 2 consecutive ECGs which taken at least 7 days apart according to the guideline.13) Transthoracic echocardiography was performed to assess the size and function of the cardiac chambers and the presence of valvular heart disease (VHD). All measurements and functional assessments of each chamber and valve were made according to the practice guideline of the major echocardiography societies, and the results were confirmed by an imaging specialist.14) Moderate to severe left atrial enlargement was defined as left atrial anterior posterior diameter of ≥47 mm in men and ≥43 mm in women, according to the aforementioned guideline.
MPI was performed using thallium-201 as a radioactive tracer according to a standardized protocol. MPI was acquired during adenosine-stress and post-stress period with a 2-head gamma camera. A perfusion defect of >10% of the total myocardium in the MPI was determined to be clinically significant, because this threshold is large enough to assign a patient to the high-risk group.15) Two clinical risk scoring systems—the revised cardiac risk index (RCRI) and the CHA2DS2-VASc score—were used according to their original definitions to determine the additional clinical implications of preoperative AF.12)16) The definition of high-risk surgery was in line with the definition in the RCRI (i.e., intraperitoneal, intrathoracic, or suprainuninal vascular procedures). The medication status just before the admission for surgery, including regular anticoagulation, were gathered. The decision for withholding anticoagulation or application of heparin bridging were made by the attending surgeon.
All study data were acquired from the Asan BiomedicaL research Environment (ABLE) system, which is a big data solution that provides anonymized form of all medical information recorded at our institution, including electronic medical records, medications, laboratory or imaging findings, and surgical records. The researchers had access to the information under the approval of the Institutional Review Board.
Study outcome
The primary study outcomes was the rate of MACCE (composite of death, ischemic strokes, and myocardial infarctions [MIs]) during the immediate postoperative period (before discharge or ≤30 days after the index surgery). The secondary outcome was the rate of ischemic stroke during the same period. The date and cause of death were recorded by an independent researcher blinded to the study group assignment. Ischemic stroke was defined as an acute episode of focal or global neurological dysfunction by ischemic injury of the brain, spinal cord, or retinal vasculature.17) Diagnosis of ischemic stroke was primarily based on diffusion-weighted magnetic resonance imaging (MRI) and clinical presentation. All the postoperative brain MRI images taken in the hospitalization for surgery were reviewed and the diagnosis of the ischemic stroke was verified by independent neuroradiologists. The MRI imaging in the perioperative period was performed in 4.8% (1,268/26,501) of sutduy population, based on the clinical symptom and signs of ischemic stroke as well as attening surgeon or nerologist's discretion. Diagnosis of MI was made primarily based on elevation of the cardiac enzyme (creatine kinase-myocardial band) or troponin I to above the upper range limit with ischemic symptoms, ECG changes, and other invasive or non-invasive investigations according to the third universal definition of MI.18) All clinical outcomes were verified and adjudicated by an independent researcher.
Statistical analysis
All statistical analyses were performed using R software version 3.3.1 software (R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org). All p values were 2-sided and p values <0.05 were considered statistically significant. Continuous variables are presented as either means with standard deviation or median values with interquartile ranges. Categorical variables are presented as frequency and percentage. Continuous variables were compared using Student's t-test or Wilcoxon rank-sum test, and categorical variables using χ2 test or Fisher's exact test, as appropriate.
Multivariable logistic regression was used to determine the independent predictors of outcome variables. The baseline characteristics of the patients and results of cardiac evaluations with clinical relevance were selected as potential risk-adjusting variables. Variables with p values <0.10 in the univariable analysis or with clinical relevance were included in the multivariable analysis. The model calibration was assessed using the Hosmer-Lemeshow test. We made two types of multivariable models to validate the pre-existing risk stratification models and assess the consistency of implication of AF to the study outcomes. In model 1, components of the pre-existing models (RCRI for MACCE; CHA2DS2-VASc score for stroke) were individually included in the multivariable model. In model 2, risk stratification score (RCRI and CHA2DS2-VASc) were included to assess the increased risk according to the increment of the score. The final model was created using a backward elimination procedure. Multicollinearity was assessed using the variance inflation factor (VIF) and no significant multicollinearity was found. Incremental discriminating performance value with addition of AF to the preexisting models was assessed using the receiver-operating characteristics (ROC) analysis. Pairwise comparisons between ROC curves were made using the method of Delong.
RESULTS
From March 2009 through December 2016, a total of 327,216 patients underwent surgery at our center (Figure 1). Among those patients, 26,501 (8.1%) underwent comprehensive cardiac evaluation within 1 year before surgery; AF was found in 1098 patients (4.1%), approximately two-thirds of whom had persistent/permanent AF (n=709, 65.6%) and another one-third had paroxysmal AF (n=389, 35.4%). The baseline characteristics of the symptomatic and asymptomatic patients are shown in Table 1. Patients with AF generally had higher clinical risk profiles such as a higher mean age, higher prevalence of hypertension, chronic lung or kidney disease, prior stroke, heart failure, MI, and peripheral artery disease. The higher risk profiles resulted in a significantly higher revised cardiac risk index as well as higher CHA2DS2-VASc score. Distribution of the surgery type showed some differences, but the rate of high-risk surgery was similar between the two groups.

Table 1
Baseline characteristics

Values are expressed as mean±standard deviation or number (%).
AF = atrial fibrillation; BMI = body mass index; LV = left ventricle; MI = myocardial infarction; RCRI = revised cardiac risk index; TIA = transient ischemic accident; VHD = valvular heart disease.
*Except mitral stenosis or prosthetic valves.
In the myocardial perfusion scan, presence of reversible defect did not significantly differ between the 2 groups, but ischemic burden (≥10%) was more common in patients with AF. Baseline echocardiography showed that patients with AF had larger left atrium, left ventricular (LV) end-diastolic dimension, higher rate of moderate-to-severe VHD, and lower mean LV ejection fraction. Medications related to AF management such as antiplatelets, anticoagulants, beta-blockers, and calcium channel blockers were more frequently prescribed in the AF group.
During the 30 days after the index surgery, MACCE and ischemic stroke occurred in 353 (1.3%) and 122 (0.5%) patients, respectively (Table 2). In the crude analysis, the patients with AF had a significantly higher rate of MACCE (4.6% vs. 1.2%, p<0.001) and ischemic stroke (1.4% vs. 0.4%, p<0.001, Figure 2). Chronic anticoagulation therapy and heparin bridging therapy were prescribed in 350 (31.9%) and 73 (6.6%) patients with AF, respectively. The rate of MACCE (2.7% [2/73] vs. 2.9% [8/277], p=0.946) or ischemic stroke (0% [0/73] vs. 1.4% [4/277], p=0.584) did not significantly differ between patients with heparin bridging and those without. Of those AF patients with ischemic stroke (n=15), 11 patients (73.3%) did not receiving anticoagulants and 4 patients (26.7%) taken anticoagulants before surgery but temporarily withheld at the time of ischemic stroke.
Table 2
Crude event rates according to the presence of AF and risk stratification
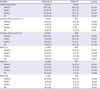
Figure 2
Rate of MACCE (A) and ischemic strokes (B) during the immediate postoperative period.
AF = atrial fibrillation; MACCE = major adverse cardiac and cerebrovascular events.

The predictors of MACCE according to univariable and multivariable analyses are summarized in Table 3. In the univariable analysis, preoperative AF (odds ratio [OR], 3.95; 95% confidence interval [CI], 2.88–5.31; p<0.001) was associated with significantly higher odds of postoperative MACCE, together with all components of RCRI and variables from non-invasive risk stratification evaluations. The higher odds of AF (OR, 2.96; 95% CI, 2.11–4.08; p<0.001) for MACCE was consistent in the final multivariable model 1, after backward-elimination procedure. The AF was also an independent predictor of MACCE in the model 2, in which the RCRI itself was included as a continuous variable. There was a differential implication of AF on MACCE when the patients were stratified according to the RCRI (Figure 3). AF was associated with a higher odd for MACCE for all RCRI groups, but the OR was higher in the patients with a lower RCRI (OR, 2.11; 95% CI, 1.17–3.56; p= 0.007 for ≥2 RCRI risk factors; OR, 3.34; 95% CI, 2.04–5.20; p<0.001 for 1 RCRI risk factor; OR, 6.35; 95% CI, 3.32–11.27; p<0.001 for no RCRI risk factor; p for interaction=0.010).
Table 3
Predictors of postoperative major coronary and cerebrovascular events

Figure 3
Rate of MACCE by the AF status, stratified by the revised cardiac risk.
AF = atrial fibrillation; CI = confidence interval; MACCE = major adverse cardiac and cerebrovascular events; OR = odds ratio.

The same procedure was performed for secondary outcome of ischemic stroke (Table 4). The preoperative AF was significant predictor in univariable analysis (OR, 3.27; 95% CI, 1.83–5.46; p<0.001) and multivariable model 1 (OR, 1.92; 95% CI, 1.01–3.43; p=0.036) adjusted for the components of CHA2DS2-VASc score and result of evaluations. The AF was also an independent predictor of ischemic stroke in the model 2 (OR, 2.30; 95% CI, 1.27–3.89; p=0.003) in which the CHA2DS2-VASc score itself was included. When patients were stratified according to the CHA2DS2-VASc score, a higher stroke rate of AF patients was noted only in those patients with a CHA2DS2-VASc score ≥2 (1.7% vs. 0.5%, p<0.001, Figure 4). The rate of a stroke was almost negligible in the patients with lower CHA2DS2-VASc scores (0–1, 0% vs 0.2%, p=0.718), regardless of the AF status.
Table 4
Predictors of ischemic stroke
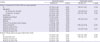
Figure 4
Rate of ischemic strokes by the AF status stratified by the CHA2DS2-VASc score.
AF = atrial fibrillation.

We assumed that the AF has as much influence as 1 point of RCRI (for MACCE) or CHA2DS2-VASc score (for ischemic stroke), since OR of AF were similar to that of 1-point increment of each scoring system (Tables 3 and 4). In the ROC analysis, addition of AF to the RCRI significantly enhance the discriminating performance (area under curve [AUC] 0.667 [95% CI, 0.640–0.693] to AUC 0.688 [95% CI, 0.662–0.714], p<0.001, Supplementary Table 1 and Supplementary Figure 1). However, for ischemic stroke, addition of AF to the CHA2DS2-VASc score showed only trend of enhanced discrimination without statistical significance (AUC 0.733 [95% CI, 0.685–0.781] to AUC 0.739 [95% CI, 0.690–0.787], p=0.165).
DISCUSSION
In this retrospective study, we report significant findings regarding the implication of AF with respect to perioperative cardiovascular outcomes: 1) preoperative AF was an independent risk factor of MACCE and ischemic stroke, independent of the prior risk evaluation systems and cardiac evaluation results; 2) relative contribution of AF status to MACCE was the largest in patients with low RCRI; and 3) the discriminating performance of RCRI was significantly enhanced by the addition of AFs.
The risk of supraventricular arrhythmias, which was included in the original cardiac risk index,19) was eliminated in its revised version for subsequent studies indicated a lower level of risk.12) Nevertheless, considering the increasing prevalence of AF and the advancement in the prevention methods against AF-related complications, the clinical implication of preoperative AF is being highlighted. Kaatz et al.6) demonstrated an increased risk of stroke in patients with AF, and van Diepen et al.20) showed that AF patients had a higher risk of mortality compared with coronary artery disease patients. Although these studies have epidemiologic implications outcomes were not adequately adjudicated in these analysis of claim data based studies. McAlister et al.10) showed that AF patients had a higher risk of stroke by directly assessing stroke outcomes from prospective registry data; however, the authors did not sufficiently incorporate the data from preoperative cardiac evaluations. In this regard, our study has major advantages over prior studies in the following regard: as the main outcome of ischemic strokes was directly assessed from imaging studies, our study provides a more precise incidence of the outcomes than did the previous studies; in addition, as we analyzed patients who underwent comprehensive cardiac evaluations, we were able to incorporate the clinical implication of these evaluations, which were not incorporated in prior risk stratification systems. Taken together, our study is an important extension of prior studies that examined the independent clinical implications of AF in cardiac and cerebrovascular outcomes.
The association between AF status and perioperative overall MACCE was not well-evaluated in prior studies, although the association between myocardial injury after non-cardiac surgery and AF was demonstrated in the Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) study, whose results are in line with our findings.21) Such association may be partially explained by decrease in cardiac output from the loss of the atrial contraction and decrease in ventricular filling time, which may be exaggerated by surgical stress.22) Our results showed that AF was an independent predictor of MACCE and significantly increased the discriminating performance, even with the consideration of the established risk scores and cardiac evaluations. In addition, a subgroup analysis demonstrated that the odd ratio of AF was the highest in patients with lower RCRI risks. This reversed trend implies that the contribution of AF on MACCE is diluted in patients with multiple risk factors, but maximized in those without risk factors. Therefore, our study demonstrates that AF has clinical utility in defining the high-risk patients, especially in those with lower clinical risk scores; thus, we suggest that AF be incorporated in peri-operative risk stratification.
In our analysis, both CHA2DS2-VASc score and AF were significantly associated with perioperative ischemic stroke. Defining high-risk group for ischemic stroke is of clinical significance as the rate of perioperative ischemic stroke is increasing, which is in contrary to the decreasing rate of MI or overall mortality.4) Our finding implies that the CHA2DS2-VASc score could be used for assessing the risk of stroke in not only AF patients but in overall population as well. Specifically, the negligible rate of ischemic stroke in patients with low CHA2DS2-VASc scores (0–1) indicates that this group should be designated as a truly low-risk group. On the contrary, AF may be used as a useful marker for high-risk group for ischemic stroke, considering its independent association with both cardiac and non-cardiac comorbidities as well as higher CHA2DS2-VASc score. Therefore, although the addition of AF did not significantly enhance the discriminating performance, our results suggest that the presence of preoperative AF may have clinical utility in refining risk assessment.
There were several limitations in this study. The retrospective observational design of the study entails inherent selection bias. As all patients enrolled in the analysis were those whom functional capacities cannot be measured or with clinically risk factors, the study population was fundamentally high-risk patients assessed by the attending surgeons. Therefore, generalization of the current findings should be done with caution as it could be a selected high-risk population. As the patients were enrolled over 10 years of period, indication for the anticoagulation was not consistent which could influence the study outcomes. As the current analysis was in retrospective nature, although general principle of preoperative evaluations of our center was given, detailed indications of each evaluation cannot be fully assessed. In its original description, the targeted outcome of RCRI was not MACCE or ischemic stroke; however, as both main study outcomes had been commonly used in recent studies, our findings still hold clinical significance. Lastly, although we analyzed a relatively large-sized population, we could not develop a new prediction model because the number of clinical events was small. The small number of events also led to the limited number of significant predictors in the final multivariable models.
In conclusion, preoperative AF was a clinically important independent predictor of peri-operative MACCE and ischemic stroke. We suggest that preoperative AF be incorporated into future risk assessment models in order to better predict cardiovascular events after non-cardiac surgery.
 XML Download
XML Download