

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
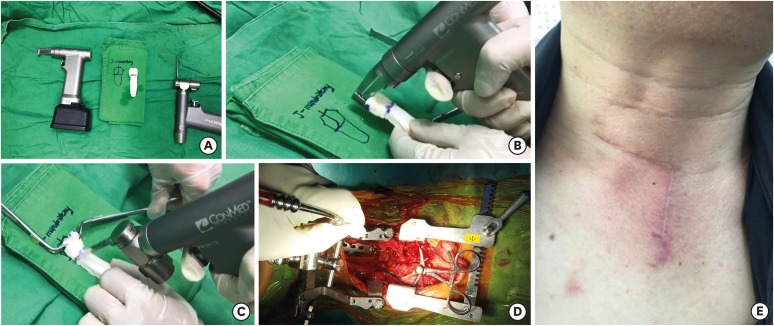
The cervicothoracic junction is usually defined by many authors as an area extending from C7 to T4.1113) Anterior approaches to the cervicothoracic junction remain challenging because of the vital vascular and neural structures and osseous obstacles over the operative field.10) To reach the upper thoracic vertebrae, many extensive approaches have been proposed combining thoracotomy, sternotomy, or clavicle resection with anterior dissection into the superior mediastinum. Previously reported anterior approaches to the cervicothoracic junction have described the full trans-sternal approach, the transclavicular transmanubrial approach and transmanubrial approach.12121318) However, it is clear that wide splitting the sternum or resecting part of the clavicle, manubrium might cause complications such as chronic pain, sternal dehiscence, nonunion of the clavicle, pseudoarthrosis, and instability of the sternoclavicular.814) In order to reduce surgical complications, we attempted to use modified anterior approach to the cervicothoracic junction in 6 patients with cervicothoracic junction lesions.(TABLE 1, FIGURE 1)
TABLE 1
Patient demographic data

CASE REPORT
Case 1
A 70-year-old female was admitted with upper back pain and shoulder pain after slip down. She had quadriparesis (both arm 4/5, both leg 3/5) and hypesthesia below T1 dermatomes.
The computed tomography (CT) scan revealed T1 burst fracture (FIGURE 2A). Under general anesthesia, the patient was placed supine with the neck extended slightly and rotated to the right. An incision was made and extended to the lower cervical vertebra by using the anterior approach. First, the sternum and the clavicle were exposed, and then the medial portion (up to one-third) of the clavicle and part of the sternal manubrium were splitted with retractor after sternal manubriotomy. By using a raspatory all procedures were safely done when the periosteum was separated from the bone. The procedure of separation was extended caudally to expose the level of the lesion, the aortic arch and the great vessels were retracted to the right side without direct separation. The patient underwent corpectomy on the first thoracic vertebra and reconstruction was done with fibular allograft and anterior plate. Steel wires were used to close the sternal manubrium. The left sternal branch of the sternocleidomastoid muscle was sutured to the interclavicular ligament. The periosteum of the exposed clavicular region was densely sutured to the costoclavicular ligament (FIGURE 2B). There was no associated morbidity and complication.
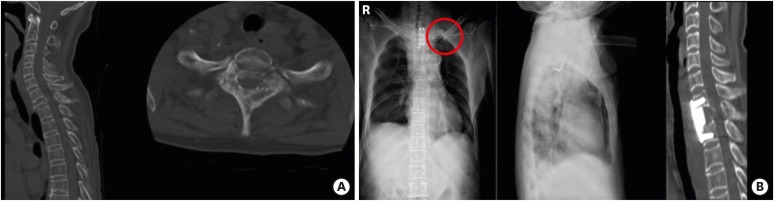
FIGURE 2
The computed tomography (A) revealed T1 burst fracture. The patient was treated with modified transclavicular transmanubriotomy with cervical incision and corpectomy was performed on the first thoracic vertebra and reconstruction was done with fibular allograft and anterior plate from C7 to T2 and the left clavicle was reapproximated (red circle) (B).
Case 2
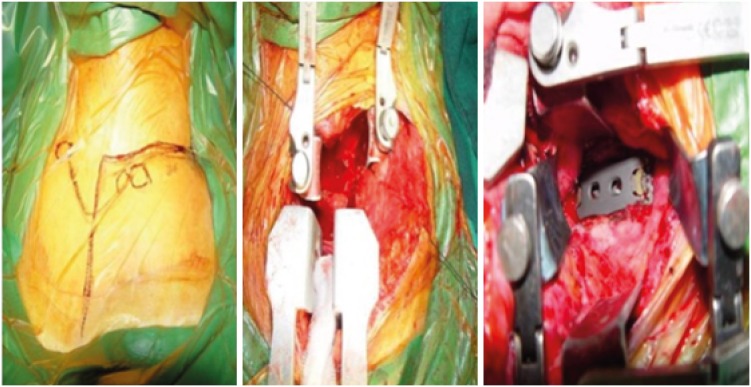
A 33-year-old male was admitted to the hospital with slight drowsy mentality after a traffic accident as a pedestrian. Initially, the patient presented upper back pain with no motor and sensory neurologic deficits. Initial CT and magnetic resonance imaging (MRI) showed stable vertebral body fracture on T1 (FIGURE 3A & B). After 2 weeks, the patient started ambulation and physical therapy. After ambulation, the patient progressively complained of severe shoulder and upper back pain. Symptom aggravation followed and the patient developed paraparesis (arm 3/5, leg 2/5). Pathologic reflexes such as Babinski sign and ankle clonus were positive. Hypesthesia was checked below T1 dermatomes. The CT and MRI showed dislocation in C7/T1 level and signs of cord compression (FIGURE 3C & D). We decided to operate the patient. To allow cervical extension the patient was placed in supine position and a small size sand bag was placed underneath the shoulders. The head was slightly turned to the right side. On the left side, the skin incision was made from the anterior border of sternocleidomastoid muscle toward the distal part of sternal manubrium (FIGURE 4). The platysma was excised and the sternocleidomastoid muscle was divided at the point of attachment. Separation of the sternothyroid and sternohyoid were done. Muscles attached to the medial half of the clavicle were subperiosteally detached. Retrosternal fat tissue and thymus were isolated by dissecting them bluntly. The inferior thyroid artery and vein may be ligated. Manubriosternotomy was performed with a gigli saw and sternotomy saw. After bleeding control, the thoracic retractor was used to spread open the rib cage gently, and caspar retractor was placed to protect the trachea and esophagus medially, and the carotid sheath and left subclavian vessels laterally and the brachiocephalic vein caudally. The pleura and left common carotid artery were moved laterally. After corpectomy of the T1 body, C7–T1 interbody graft using titanium mesh cage filled with allograft bone chips and anterior plate system were successfully achieved (FIGURE 3E). Closure was done after irrigation, hemostasis and placement of a deep drain. Stainless steel wires were used to close the sternum. The interclavicular ligament and the left sternal branch of the sternocleidomastoid muscle, which was separated from the sternal manubrium, was sutured together. Closure of the platysma, subcutaneous tissue and skin wounds were done routinely.
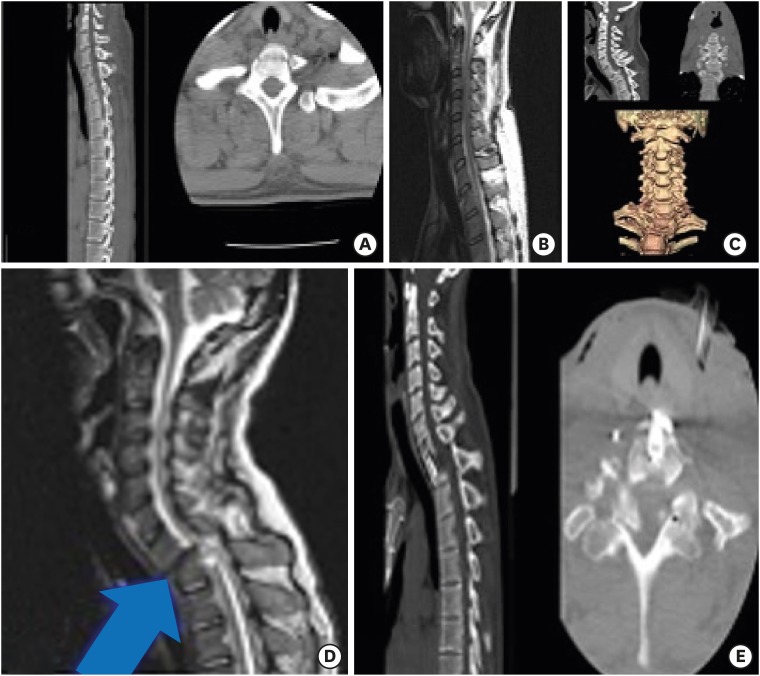
FIGURE 3
He had a traffic accident. His ASIA score was A. Initial CT showed stable vertebral body fracture in T1 (A). Sagittal T2 weighted MRI showed no cord signal change in cervicothoracic level (B). After paraparesis, CT and 3-dimensional CT revealed anterior dislocation and translation C7 on T1 and kyphotic angulation was observed (C). Sagittal T2 weighted MRI revealed diffuse cord signal change in C7/T1 area due to dislocation (blue arrow) (D).Postoperative CT showed T1 median corpectomy and reconstruction with titanium mesh andanterior plate from C7 to T1 via modified anterior transmaubriotomy (E).
CT: computed tomography.
DISCUSSION
Lesions in the cervicothoracic junction are not rare, but surgical exposure of this region remains challenging. The anterior sternotomy approach to the cervicothoracic junction requires exact knowledge of the surgical anatomy, skill and careful planning according to the pathology in this region. This is especially true for commonly needed anterior approach lesions in the vertebral body. However, the kyphosis of the upper thoracic spine make the vertebral bodies hard to locate due to its depth, and the presence of neurovascular and osseous obstacles limit the surgical approach.6101115) To decrease the surgical risk, a thoracic surgeon may aid exposure. In our institute we performed this approach together with a thoracic surgeon for safety and to reduce operation time. Injury to the brachiocephalic veins, thoracic duct, and recurrent laryngeal nerves, may lead to significant complications.13) The best method is to reach the spine through neurovascular space, and to bypass them. Surgical access is not always limited by osseous obstacles. If simple access to T1 and upper levels is required, the traditional anterior low cervical approach can be enough. However, traditional anterior low cervical approach limits additional work field for procedures such as anterior plating, corpectomy because of the anterior bony structure. Previous authors have mentioned such problems.6) The sternal manubrium and clavicles often interrupt access to the upper thoracic level (T1–T3). Surgical techniques such as the transsternal, the transclavicular-transmanubrial and transmanubrial approaches have been recommended to gain access. Each approach has its advantages, but limitations exist in all of them. Fielding and Stillwell5) first reported the anterior low cervical approach to cervicothoracic junction in 1976, but an exposure caudal to T2 is usually limited by sternal manubrium and clavicles. Cauchoix and Binet2) first described a full median sternum-splitting approach, for T1–T3 in 1957. Hodgson et al.7) reported that they had performed median sternotomy in upper thoracic tuberculosis spondylitis in 1960. Sundaresan et al.16) suggested a transclavicular-transmanubrial approach for improving exposure and providing a strut graft in 1984. A modified transmanubrial approach was used by Darling et al.3) and by Xiao et al.18) T4, and occasionally T5 can be accessed by this technique. However, a relatively narrow access to the spine is provided (a width of no more than 4 cm).6) For more working room of this area, Luk et al.15) used bilateral manubriotomy. This technique could provide a width of approximately 8 cm, but transverse osteotomy of the sternum and ligations of the bilateral internal thoracic arteries is needed.
In our case, we used 2 modified anterior cervicothoracic approach methods. We performed a modified transmanubriosternal approach combined with a standard cervical incision (Smith-Robinson approach) in one case and a modified transsternal transclavicular approach with standard cervical incision in another case. Both approach provided the same surgical field. To decide the surgical approach pre-operative radiologic evaluation must be done to determine the extent of surgery and to anticipate the surgical field. We used three guidelines for pre-operative radiologic evaluation. The Teng guideline determined the extent of operation based on the lesion location using the Cervicothoracic angle as the standard.17) The Karikari guideline also determined the extent of operation using the intervertebral disc line as a standard.9) The Falavigna guideline was used to determine the extent of surgery and also anticipate the surgical field using the Surgeons' view line.4)
With our experience, we recommend the modified transmanubriosternal approach combined with a standard cervical incision. This procedure is somewhat simple to perform, requires little additional operative time for opening or closure. It provides excellent operative field view. The regional anatomy is also familiar to neurosurgeons. There is no associated severe complication and comorbidity related to this approach.
CONCLUSION
Pre-operative radiological evaluation identified the cases in which manubriostomy was necessary. The modified transmanubriosternal approach combined with a standard cervical incision is technically simple to perform. It also provides excellent exposure to the cervicothoracic junction from C3–T4 without having to perform a full median sternotomy. It also helps avoid injury to subclavian vessels due to resection of the clavicle or sternoclavicular junction. There is less severe complication and comorbidity which results from the extent of the surgery.
 XML Download
XML Download