

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Transient global amnesia (TGA) is an acute neurological self-limited disorder characterized by a sudden onset anterograde short termed amnesia.1 Posterior reversible encephalopathy syndrome (PRES) is a clinico-radiological syndrome that comes with seizure, headache, altered mental status, and visual disturbance.2 Although PRES can have various clinical presentations, cognitive decline that appears to be TGA has not yet been reported in a Korea patient with PRES. This study looks into a patient whose clinical course resembled TGA, but whose radiological findings were compatible with PRES. This study was approved by the Institutional Review Board of the participating hospital, and obtained patient consent.
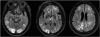
This study is about an 81-year-old female patient with 12 years of education with acute memory disturbance and headache but without altered mental status. She had suffered from hypertension for a period of 1 year but had stopped taking her antihypertensive medication 2 months earlier. She all of a sudden began to behave strangely and was brought to the emergency room by her daughter 3 hours later. She was alert and communicative, and her personal identity was preserved. However, she did not remember the combination for her door lock and repeatedly asked her family the same question. In the emergency room, she complained of a mild headache, but denied any visual disturbance. The physical examination was normal, except for the blood pressure, which was 212/97 mmHg. Her body temperature was normal, and there was no evidence of infection. In the neurological examination, she was alert and oriented with regard to person and place but not to time. She could not acquire new information or recall events that had occurred that day or the previous one. She repeatedly asked the same questions, such as “Where am I?” and “Why am I here?” However, her speech, reasoning, and remote memories were intact. Motor and sensory functions and cranial nerve examination showed no abnormality. The initial laboratory tests showed mild leukocytosis (14,300/mm3), but otherwise were normal. The cerebrospinal fluid analysis was within normal range except a high protein level of 126.4. The Korean version of Mini-Mental Status Examination (K-MMSE) score was 18/30. She had low scores, 2/5 for time orientation score, 1/5 for place orientation score, and 0/3 for delayed recall. However, immediate recall, calculation and language scores were in the normal range. Electroencephalography was normal with no epileptiform discharge. Brain magnetic resonance imaging (MRI) revealed high-intensity signal changes in several subcortical areas, particularly the parieto-occipital regions, on diffusion-weighted imaging and fluid-attenuated inversion recovery images (Fig. 1). She was treated for hypertension with intravenous nicardipine, and her blood pressure normalized (135/68 mmHg). By the next morning, she had recovered from her amnesia and confusion, although there was a gap in her memory for the episode. Her headache had also decreased, and there were no neurological deficits. Three months later, a follow-up MRI showed that all of the occipito-parietal subcortical white matter lesions had disappeared, and the score of K-MMSE rose to 28/30. She was finally diagnosed with PRES due to severe hypertension.
Both TGA and PRES are acute neurological disorders common in neurological emergencies. TGA is a heterogeneous clinical syndrome characterized by the abrupt onset of profound anterograde amnesia with repetitive questioning that lasts up to 24 hours. The patients remain alert, communicative and with an intact personal identity during the attack. The cognitive impairment is limited to amnestic period, and there are no clinical sequelae.34 The pathophysiology of TGA is uncertain, although the widely accepted hypothesis is that it is caused by thromboembolic cerebrovascular disease involving the hippocampal parenchyma.56 The symptoms in the 81-year-old female patient met the diagnostic criteria for TGA clinically. However, MRI showed no hippocampal involvement, but diffused white matter sub-cortex lesions. It is very similar to PRES image findings. PRES is a clinic-radiological syndrome with a unique pattern of brain vasogenic edema involving the white matter of both posterior cerebral hemispheres.789 Vasogenic edema results from auto-regulatory failure caused by conditions such as severe hypertension, massive transfusion, cancer chemotherapy, and infection. The symptoms of PRES are non-specific and can manifest as a variety of neurological disorders such generalized tonic-clonic seizures, headache, and visual disturbances among others.210 The symptoms and signs of PRES have a wide range of severity and there are no guidelines to direct their assessment. Therefore, the diagnosis of PRES requires brain imaging, although clinical context is crucial to making the correct diagnosis.2 The 81-year-old female patient also clinically appeared to have TGA, but the radiological findings suggested PRES. The malignant hypertension, over 200 mmHg, supported the diagnosis of PRES. Therefore, this is the unique case of PRES appearing as TGA. This study established that PRES should be considered in the differential diagnosis of TGA because cognitive decline can be the first symptom of PRES.
 XML Download
XML Download