

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative internal herniation is the protrusion of a viscus through a mesenteric or peritoneal aperture [1]. Abdominal pain followed by nausea and vomiting is the most common symptom of internal hernia [2]. Roux-en-Y and Billroth-II reconstructions in gastrectomy contribute to the dominant cause of internal hernia[34]. The overall frequency of internal hernia after total gastrectomy was 0.14% and higher after laparoscopic surgery than after open surgery. Hiatal hernia is a type of internal hernia and is a rare complication, occurring in only 0.01% of total gastrectomy cases [2]. We report a rare case of incarcerated hiatal hernia with perforation after total gastrectomy with Roux-en-Y reconstruction.
CASE REPORT
A 76-year-old man with a history of type 2 diabetes mellitus, hypertension, old cerebrovascular accident, and spinal stenosis. He presented with anemia and tarry stool initially. Upper gastrointestinal (UGI) panendoscopy and abdominal computed tomography (CT) revealed a submucosal tumor, consistent with gastrointestinal stromal tumor, so he was regularly followed up at the gastrointestinal outpatient department. However, stool occult blood positive with anemia was still found 3 months later, but no tarry stool, poor appetite, nausea, vomiting, abdominal pain, or body weight loss was found. Owing to the aforementioned, UGI panendoscopy was performed again, which showed a hyperemic area at the posterior wall of the high body to the cardia and a submucosal mass, approximately 1.8 cm, with tiny erosions at the lesser curvature side of the antrum. In addition, no preoperative hiatal hernia was found (Fig. 1). The biopsy of the high body showed a poorly cohesive carcinoma. Then, an abdominal CT scan disclosed a gastric polypoid tumor, approximately 1.5 cm, with penetrating subserosal connective tissue without invasion of the visceral peritoneum or adjacent structures, cT3N0M0, stage IIA. Thus, preoperative peripheral parenteral nutrition support was provided, and then laparoscopic total gastrectomy with Roux-en-Y anastomosis in the ante-colic route and D2 lymphadenectomy were performed. An extra 1-cm esophagectomy above the gastroesophageal junction was also performed for the equivocal frozen pathology without mediastinal lymph node dissection. No intraoperative complications were observed, and the hiatus was not opened wide during the surgery, in which the crus muscle was transected by dividing the phrenoesophageal membrane only for creating enough space for the side-to-side esophagojejunostomy (EJS) anastomosis using a linear stapler(Endo-cuter J&J, 45–3.5; Fig. 2). The common entry hole was then closed using an intracorporeal continuous suture of 3-0 V-Loc, and the final pathological report was poorly cohesive carcinoma, pT4aN1M0, stage IIIA, with a clear surgical margin.
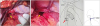
Fig. 1
Preoperative upper gastrointestinal panendoscopy. (A, B) The arrow indicates the hyperemic area at the posterior wall of the high body to the cardia. (C) The arrow indicates the submucosal mass at the lesser curvature side of the antrum. No preoperative hiatal hernia was observed.


Five days later, follow-up chest radiography demonstrated a hiatal hernia over the left chest (Fig. 3). As the postoperative course was uneventful, the hiatal hernia was followed up with observation. The patient gradually started water intake, a liquid diet, and a soft diet. However, 8 days after the operation, he presented with poor appetite and abdominal fullness, which progressed to vomiting, dyspnea, and high fever (39.5°C). A laboratory examination revealed a white blood cell count of 20,300/μL and C-reactive protein level of 19.2 mg/dL. The chest-to-abdominal CT scan demonstrated a disruption of the left-side diaphragm, with a severely distended small bowel herniation into the left pleural space and massive pleural effusion (Fig. 3). A diagnosis of incarcerated hiatal hernia was made, and emergent exploratory laparotomy was performed. Intraoperative findings revealed the herniated Roux limb through the defect on the diaphragmatic hiatus into the left pleural cavity with massive pleural effusion and food material (Fig. 4). The incarcerated intestine was drawn back into the abdominal cavity safely. A transient ischemic change of the Roux limb was observed, which improved after reduction. Unfortunately, EJS leakage and perforation of the small intestine, 20 cm above the jejunojejunal anastomosis, were also found. The perforated intestine was repaired using a linear stapler (Endo-cuter J&J, 45–3.5), the EJS anastomosis was reinforced for poor healing with a 3-0 silk suture, the crus was approximated with 2 figure-8 sutures, and the diaphragm was repaired with 1-0 Prolene suture (Fig. 4). Feeding jejunostomy was performed for nutrition support. Moreover, for the left pyothorax and EJS leakage, thoracoscopic decortication of the left chest and esophagostomy with T-tube diversion were performed. Then, the patient was transferred to the intensive care unit for postoperative monitoring.
Fig. 3
(A) Chest radiograph showing the intestine in the left lung field. (B) Abdominal computed tomography image showing distended loops of the small intestine in the left thoracic cavity.

Fig. 4
Intraoperative finding showing the orifice of the hernia (yellow arrow). The red arrow indicates the crural approximation.
Enteral nutrition via a jejunostomy tube begun on postoperative day 1. Bacteremia and fungemia were found later, but after antibiotic treatment and intensive care, he recovered well except for a mild residual empyema. In addition, the esophagogram showed no anastomotic leakage and no recurrent hiatal hernia (Fig. 5), so oral intake was started. Then, he was discharged after 92 days of hospitalization under a stable condition.
Fig. 5
(A) The latest chest radiograph. (B) The latest esophagogram showing no recurrent hiatal hernia before hospital discharge.

At the latest follow-up, the patient had a fall event that caused an intracranial hemorrhage and sudden-onset desaturation several days later, which caused his death.
DISCUSSION
The incidence of post-gastrectomy complications in patients with gastric cancer that require a second operation is rare. The most common causes include dehiscence, bleeding, mechanical ileus, and perforation [5]. Internal herniation after gastrectomy for gastric cancer is extremely rare and found mostly after gastric bypass for obesity. It often occurs after specific reconstructions such as Roux-en-Y and Billroth II reconstructions, probably because of the multiplicity and large size of the iatrogenically induced artificial apertures [134]. A previous study of randomized trials for comparison between laparoscopic and open surgeries in gastric cancer showed a difference in the incidence rate of internal hernias [67]. The incidence rate of internal hernia was higher with laparoscopic surgery than with open surgery. The most common presentation of internal hernia was abdominal pain, followed by nausea and vomiting [2]. In Roux-en-Y reconstruction after total gastrectomy, the potential hernia locations included the jejunojejunostomy mesentery defect, the dorsum of the Roux limb (Petersen's space), the transverse mesocolon defect, the esophageal hiatus, and the potential space between the mesentery of the ascending Roux limb and the transverse mesocolon [8]. Hiatal hernia is rare and most often mentioned after esophagectomy [910], in approximately 0.69% of cases [11]. In a Japanese study, of 8,938 patients with gastrectomy for gastric cancer, only 13 were diagnosed as having an internal hernia (0.19%) and only 1 was considered as having a hiatal hernia (0.01%) [2]. The proposed causes of hiatal hernia were negative intrathoracic pressure, resection of the diaphragmatic crus, and liver cirrhosis, which is because the esophageal hiatus, is commonly covered by the left lateral segment of the liver [12]. The cause of iatrogenic hiatal hernia is most likely blunt dissection of the hiatus during operation, which enlarges the hiatus[131415].For advanced gastric cancer of the cardia that has invaded <3 cm of the lower esophagus, left thoracoabdominal incision is not recommended [16]. In addition, regarding the substantial length of the esophagus for EJS anastomosis, although the linear stapler requires a longer esophagus with a divided phrenoesophageal membrane than the circular stapler, the incidence of postoperative complications was lower and similar between the 2 groups, indicating that the linear stapler is a safe and feasible technique [1718]. In our patient, an extra 1-cm esophagectomy was performed because of an equivocal frozen pathology and EJS anastomosis was performed via the linear stapler, without a thoracoabdominal incision.
According to the previous study, hernia repair is required when toxic signs are found, and a transabdominal approach allows for an easy reduction of the hernia contents. With early diagnosis, the only surgical intervention required is repair of the hernia defect, which has lower morbidity and mortality. However, if diagnosis is delayed, rupture of the small intestine may occur, which leads to mediastinitis, which may be life-threatening [19]. If irreversible, ischemic necrotic tissue or perforation is found, resection and repair should be performed as necessary. In our case, the patient presented abdominal fullness with vomiting, dyspnea, and high fever initially. An incarcerated small intestine with perforation and a distended bowel loop, which caused anastomotic leakage, were found during the operation. Therefore, hiatal hernia should be considered as a differential diagnosis if the patient develops any emetic or unstable symptoms and signs.
Management of the defect in the initial operation is an important issue. The high risk of internal hernia is probably related to the abdominal spaces created after Roux-en-Y reconstruction and potential orifices for internal hernia. The greatest factor possibly affecting the incidence of internal hernia after gastrectomy is closure of the mesenteric defects [72021222324]. Therefore, because blunt dissection is the main cause of hiatal hernia, including the creation of enough space for the side-to-side EJS anastomosis with a linear stapler, the crus must be approximated for closure of the dissected defect to prevent the incidence of hiatal hernia by suturing the right crus and left crus with 1 or 2 figure-8 sutures, depending on the size of the defect. In our patient, the crus approximation was performed in the second surgery, and since then, no recurrent hiatal hernia was found.
In conclusion, incarcerated hiatal hernia after total gastrectomy with Roux-en-Y reconstruction is rare, but it should be kept in mind as a possible postoperative complication. Approximation of the crus with 1 or 2 figure-8 sutures, depending on the size of defect, may be considered in patients who had undergone laparoscopic total gastrectomy.
 XML Download
XML Download