

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The pathophysiology of rotator cuff disease has traditionally been viewed as a continuum ranging from impingement syndrome to partial- and full-thickness rotator cuff tears (12). Rotator cuff disease is considered one of the most common causes of shoulder-related disability (34). Severe shoulder pain and functional restriction due to a structural problem, such as rotator cuff discontinuity that fails to improve with conservative treatment, is an indication for rotator cuff surgery. The incidence of rotator cuff surgery has increased in western countries in recent years, with a greater proportion of arthroscopic surgeries every year (56789).
Yamamoto et al. (10) reported that full-thickness rotator cuff tear had a prevalence of approximately 20% in the general population, which increased for older patients. Therefore, rotator cuff surgery is thought to be one of the most common procedures performed by orthopedic surgeons in Asia as well, but to the best of our knowledge, no epidemiologic studies have assessed rotator cuff surgery in Asian countries. Furthermore, it is believed that rotator cuff surgeries can be easily performed not only in large tertiary hospitals or general hospitals but also in small hospitals or clinics, as arthroscopic rotator cuff surgeries are associated with low morbidity and mortality (11). However, few studies have examined the differences in the incidence of rotator cuff surgery in accordance with hospital types (12).
In this context, the objective of the present study was to investigate national trends as well as hospital type-specific trends in rotator cuff surgery in Korea based on an analysis of nationwide data acquired from the Korean Health Insurance Review and Assessment Service (HIRA). Our hypotheses were as follows. First, the incidence of rotator cuff surgery would also show a rapid recent rise in Korea, and arthroscopic surgeries would account for a high proportion. Second, rotator cuff surgery would be a popular procedure commonly performed even in small hospitals.
MATERIALS AND METHODS
Data source
The authors analyzed a nationwide database obtained from the HIRA from 2007 to 2015. In Korea, 97% of the entire population are legally obligated to enroll in the National Health Insurance (NHI) program. Patients only pay about 30% of the total medical cost to hospitals or clinics, and all healthcare providers submit claims data for inpatient and outpatient management, including diagnostic codes which classified according to the International Classification of Diseases, 10th revision (ICD-10), procedure codes, prescription records, demographic information, and direct medical costs, to the HIRA to request reimbursement for the remaining 70% of the medical cost from the NHI service. Of the remaining 3% of the population not registered in the NHI program, excluding illegal residents, most receive healthcare coverage through the Medical Aid Program. The claim data for patients covered by the Medical Aid Program are also reviewed by the HIRA. Hence, medical records of almost all newly admitted or hospitalized patients at hospitals or clinics in Korea are prospectively recorded in the HIRA data.
Data collection
The authors used ICD-10 codes and procedure codes to identify patients who received surgical treatment for a rotator cuff disease (Tables 1 and 2). Rotator cuff disease was defined to include impingement syndrome (M754) and rotator cuff tear (M751, M751.01, S434.02, S4600, S4608), and data for patients with both ICD-10 codes and procedure codes (N0935–N0938) for rotator cuff disease were extracted from the HIRA data. Patients whose data included codes corresponding to instability or a superior labral tear from anterior to posterior (SLAP) were excluded from the study (Table 1).
Table 1
ICD-10 diagnosis codes used for analysis

Table 2
Procedure codes of rotator cuff disease in Korea

We examined patient data to identify the year of surgery, age, sex, whether arthroscopic surgery was performed, hospital type for surgery, and procedure code. When health care providers perform arthroscopic surgery, they input the arthroscopic device code (N0031003) to claim costs for arthroscopic devices from the NHI service, so we determined whether arthroscopic surgery was performed based on the presence of a device code (N0031003). In Korea, health care institutions are classified as clinics, hospitals, general hospitals, and tertiary hospitals. The classification criteria are based on inpatient bed size for clinics (< 30 beds), hospitals (30 to < 100 beds), and general hospitals (≥ 100 beds), and tertiary hospitals are defined as general hospitals that are approved to provide most types of advanced medical care and treat severely ill patients with a minimum of 20 departments. In Korea, the procedure codes for rotator cuff disease were limited to 3 (N0935, N0936, N0937) until June 2014, and a new code (N0938) was added after July 2014, resulting in a total of 4 codes (Table 2). Healthcare providers could only claim costs using 1 of the 4 procedure codes. For example, when both acromioplasty and rotator cuff repair (RCR) were performed, healthcare providers could claim for the one of the higher level RCR codes (N0936, N0937, N0938), and not for the acromioplasty code (N0935). Hence, patients who undergo surgery for rotator cuff disease have only 1 procedure code, and we could not determine whether a patient who received RCR also received acromioplasty using the HIRA data.
Statistical analysis
The annual percentage changes in rotator cuff surgeries were calculated from 2007 to 2015 by using joinpoint regression analysis (Joinpoint Regression Program, Version 4.3.1.0; National Cancer Institute, Bethesda, MD, USA). In the joinpoint regression analysis, we used age-adjusted and sex-specific rates per 100,000 persons, and the 2000 U.S. population as the standard population (1314). Estimated year-specific, age-specific, and sex-specific populations were obtained from the website of the Statistics Korea (http://www.kosis.kr).
All other data sets were analyzed using SAS statistical software version 9.13 (SAS Institute, Cary, NC, USA). The correlation between the total cost of rotator cuff surgeries and the gross domestic product (GDP) was analyzed using the Spearman rank test. Univariate analyses were conducted by using t-tests. The changes in the proportion of arthroscopic surgery and open surgery in accordance with the year of surgery and age of patients (10-year age groups) were analyzed using the Cochran-Armitage trend test. Values of P < 0.05 were considered significant.
RESULTS
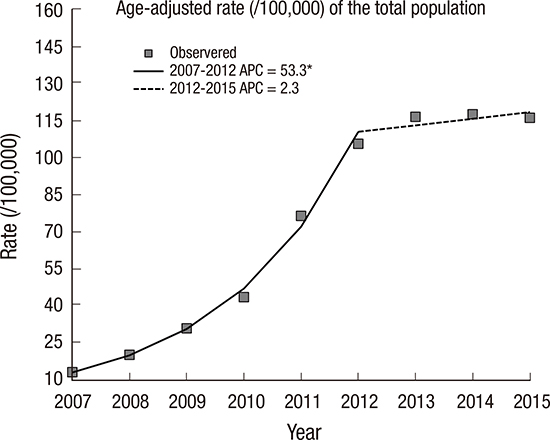
A total of 383,719 rotator cuff surgeries were performed from 2007 to 2015. Of these, 190,262 cases involved male patients, and 193,457 cases involved female patients, with a male to female ratio of 1.02. The incidence of rotator cuff surgery steadily increased approximately 11 fold from 6,771 cases in 2007 to 74,120 cases in 2015 (Table 3). The age-adjusted rate increased approximately 9 fold, from 13.15 cases per 100,000 persons in 2007 to 116.04 cases per 100,000 persons in 2015. The joinpoint regression analysis revealed a transition of annual percentage change of age-adjusted rate around 2012. The mean annual percentage change from 2007 to 2012 was 53.3% (95% confidence interval [CI] 45.0% to 62.2%), which was statistically significant with the incidence of rotator cuff surgery increasing each year compared to the previous year (P < 0.001), but that from 2012 to 2015 was 2.3% (95% CI −3.6% to 8.6%), which was not significant (P = 0.340) (Fig. 1A). Sex-specific rates demonstrated a similar trend to the total cohort (Fig. 1B, Table 4). Although the GDP in Korea only increased approximately 1.2 fold, from 1,122,679,154,632 USD in 2007 to 1,377,873,107,856 USD in 2015, the total cost of rotator cuff surgeries increased approximately 11 fold from 14,093,510 USD in 2007 to 157,805,298 in 2015 (Fig. 1C). However, there is a significant correlation the between the total cost of rotator cuff surgery and the GDP using the Spearman rank test (P = 0.002, r = 0.867).
Table 3
Number of cases and age-adjusted rates of surgery for rotator cuff disease from 2007 to 2015
Fig. 1
Age-adjusted and sex-specific rates per 100,000 persons of surgery for rotator cuff diseases and the correlation between the total cost of rotator cuff surgeries and the GDP. (A) Age-adjusted rates of the total population. (B) Sex-specific age-adjusted rates. (C) Total cost of rotator cuff surgeries and GDP in Korea.
APC = annual percentage change, GDP = gross domestic product.
*P < 0.05.

Table 4
Annual percentage change in the age-adjusted and sex-specific rate of rotator cuff surgery from 2007 to 2015
The proportion of arthroscopic surgery in all rotator cuff surgeries steadily rose from 89.9% in 2007 to 96.8% in 2015 (Table 5). The proportions were similar in male and female patients, and the trends were found to be significant through the Cochran-Armitage trend test (all P < 0.001). The mean length of hospital stay for arthroscopic surgery (11.0 days [standard deviation {SD} ± 8.0]) was significantly shorter than that for open surgery (14.5 days [SD ± 9.8]) (P < 0.001). The average total hospital cost for arthroscopic surgery (2,088 USD [SD ± 770]) was significantly higher than that for open surgery (1,904 USD [SD ± 860]) (P < 0.001).
Table 5
Percentage of arthroscopic vs. open surgery for rotator cuff disease by year
The mean age of patients who received surgical treatment for rotator cuff disease was 55.4 years (SD ± 10.8). The mean age for men was 53.4 years (SD ± 11.4), and that for women was significantly higher at 57.4 years (SD ± 9.6) (P < 0.001). In terms of age group-specific differences in the number of surgery cases, the total number of rotator cuff surgeries was highest in the 50–59-year age group (149,618 cases, 39%), followed by the 60–69-year age group (100,404 cases, 26%) and the 40–49 year-age group (73,638 cases, 19%) (Fig. 2A). However, incidence per 100,000 persons was highest in the 60–69-year age group (265.46 per 100,000), followed by the 50–59-year age group (237.44 per 100,000) and the 70–79-year age group (132.37 per 100,000) (Fig. 2B). The proportion of arthroscopic surgery tended to decrease while that of open surgery increased as age increased, and this trend was found to be significant using the Cochran-Armitage trend test (P < 0.001) (Table 6).
Fig. 2
(A) Total number of cases by age group from 2007 to 2015. (B) Incidence of surgeries for rotator cuff diseases for every 100,000 persons in that age group.

Table 6
Percentage of arthroscopic vs. open surgery for rotator cuff disease by age group

| Age group | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80+ | P value |
|---|---|---|---|---|---|---|---|---|---|
| Open | 3.3 | 2.2 | 2.3 | 2.9 | 3.7 | 5.2 | 6.9 | 12.6 | < 0.001* |
| Arthro | 96.7 | 97.8 | 97.7 | 97.1 | 96.3 | 94.8 | 93.1 | 87.4 |
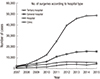
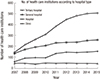
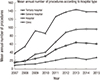
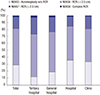
In terms of incidence according to hospital type, the highest rate of increase was in hospitals (30 to < 100 beds), where the number of cases of rotator cuff surgery increased by 19.6 times from 2,479 cases in 2007 to 48,568 cases in 2015 (Fig. 3). The number of health care institutions that performed rotator cuff surgery at least once per year increased from 379 in 2007 to 957 in 2015, of which hospitals (30 to < 100 beds) accounted for the greatest proportion (Fig. 4). The mean annual number of procedures was calculated by dividing the total number of procedures by the total number of each hospital type. The mean annual number of procedures was greatest in tertiary hospitals, followed by hospitals, general hospitals, and clinics (Fig. 5). Component ratio of types of procedure varied by hospital type, with hospitals (30 to < 100 beds) and clinics demonstrating a higher proportion of isolated acromioplasty procedure (N0935) than general hospitals or tertiary hospitals (Fig. 6).
Fig. 3
Total number of surgeries for rotator cuff disease according to hospital type from 2007 to 2015.
DISCUSSION
To the best of our knowledge, this study is the first to report national trends in the surgical treatment of rotator cuff diseases in East Asia. In Korea, the number of cases of surgical treatment of rotator cuff disease steadily rose from 2007 to 2015. The age-adjusted rate per 100,000 persons rapidly increased from 2007 to 2012 and was then maintained at a steady state from 2012 to 2015. In 2007, a large number of surgeons already preferred arthroscopic surgery, and the number grew annually, resulting in 96.8% of all rotator cuff surgeries being conducted arthroscopically in 2015. Cases of rotator cuff surgery increased by the greatest degree in hospitals with 30−100 inpatient beds, and the component ratio of procedure codes varied in accordance with type of hospital.
In the United States, the age-adjusted rate of RCR per 100,000 persons reached 103.62 cases in 2006 (6), while that in Korea in 2007—including the isolated acromioplasty procedure—was considerably lower, at 13.15 cases per 100,000 persons. However, the number of surgical treatments of rotator cuff disease rapidly increased in Korea up to 2012 (105.55 cases per 100,000 persons in 2012), reaching a similar level to that of the United States in 2006 (Fig. 1). Considering the Korean GDP per capita in 2012 (24,454 USD) compared to that of the United States in 2006 (46,437 USD) and the fact that the number of rotator cuff surgeries tends to relate to the GDP, the frequency of rotator cuff surgery in Korea in 2012 was especially high.
Such rapid escalation in the number of surgical treatments could be explained by a few possible factors. First, there has been an increase of shoulder surgeons and sports medicine surgeons who are capable of performing this procedure. Judge et al. (7) reported that the number of specialist shoulder surgeons increased by 164% from 2000 to 2010 in the United Kingdom, which subsequently resulted in a rapid increase of rotator cuff surgeries. Although the present study could not directly examine the number of surgeons, we were able to indirectly infer that the number of surgeons performing rotator cuff surgery had increased based on the fact that the number of health care institutions performing this procedure increased by 2.5 times during the study period (Fig. 4). Second, there has been a gradual shift in surgeons' preference to perform surgical treatment for rotator cuff diseases (1516). According to a report from the United States, there has been an increase in the rate of surgical treatment for rotator cuff disease, where among patients who visited hospitals or clinics for shoulder pain, there were 26 nonsurgical visits per 1 RCR in 1996, while the number decreased to 16 visits per 1 RCR in 2006 (6). Dunn et al. (16) indicated that there was a positive correlation between the volume of procedures performed by a surgeon and the surgeon's perception of outcome, with surgeons who had a higher procedure volume being more enthusiastic about rotator cuff surgery than those who had a lower procedure volume. Similarly, it is believed that the increased experience with rotator cuff surgery of surgeons in Korea may have increased their preference for surgical treatment, contributing to the rapid rise in the number of surgeries. Third, there have been improvements in diagnostic techniques used to identify tears and greater accessibility to this technology for both physicians and patients (1217). Finally, advances in arthroscopic surgery could also have contributed to the increase of surgical treatment by reducing patient burden related to surgery compared to an open surgery (18). We are not sure why the age-adjusted rate per 100,000 persons has been steady state since 2012. The incidence of rotator cuff surgeries increased rapidly up to 2012, at which time it had already reached too high of a level considering GDP. The age-adjusted rate of rotator cuff surgery appears to have plateaued after 2012.
In Korea, the vast majority of rotator cuff disease surgeries are performed arthroscopically (Table 5). Arthroscopic surgery has a number of advantages over open surgery, including smaller incision, improved ability to evaluate and treat pathology of the glenohumeral joint, improved visualization, decreased postoperative pain, and short hospital stay (19). In support of this statement, the present study also demonstrated a significantly shorter hospital stay after arthroscopic surgery (11.0 ± 8.0) compared to that after an open surgery (14.5 ± 9.8). However, despite the shorter hospital stay, arthroscopic surgery was associated with a higher cost, which is presumably due to the cost of arthroscopic devices. Nevertheless, the proportion of arthroscopic surgeries increased over the study period owing to its advantages that offset the high cost, which is similar to the trend in the United States (68).
In Korea, the incidence of rotator cuff surgery was highest in the 60−69-year age group, followed by the 50−59-year age group, and 70−79-year age group. Although elderly patients generally have a greater incidence of rotator cuff disease (10), the incidence of rotator cuff surgery declined after the age of 70. Park et al. (20) reported that the failure rate for RCR was significantly higher in patients aged > 69 years compared with those aged ≤ 69 years and retears of the rotator cuff are closely associated with advanced age (2122). Initial conservative treatments can be safely undertaken in older patients (> 70 years old) with chronic tears (4). These factors seem to result in a low incidence of rotator cuff surgery over the age of 70. Furthermore, the proportion of open surgery increased with the age of patients (Table 6), which is thought to be the result of more cases involving a large rotator cuff tear combined with a subscapularis tear in older patients (2324). Arthroscopic repair of a large rotator cuff tear combined with a subscapularis tear is known to have poor results and to be technically demanding (25). Bartl et al. (26) reported that open repair of combined tears of the subscapularis and supraspinatus tendon achieved good postoperative results. For the above reason, the proportion of open surgery is believed to increase in older patients with combined tear involving a subscapularis tear.
Hospital size-specific analysis revealed an increase in the number of health care institutions performing rotator cuff surgery, and hospitals with 30−100 beds increased by the greatest degree (Fig. 4), which contributed to the rapid increase in rotator cuff surgery (Fig. 3). The low morbidity and mortality associated with arthroscopic surgery are believed to have contributed to popularity of rotator cuff surgery in relatively smaller hospitals (11). However, there is a large gap between hospitals with 30−100 beds and clinics regarding mean annual number of rotator cuff surgeries per institution. Hospitals with 30−100 beds had higher mean annual number of rotator cuff surgeries per institution than general hospitals, even though they are smaller (Fig. 5). This phenomenon is presumably due to the fact that more hospitals with 30−100 beds specialize in the treatment of joints such as the knee and shoulder than general hospitals or clinics in Korea. For rotator cuff surgery, many patients seem to prefer hospitals specializing in the treatment of joint disease rather than general orthopaedic hospitals. In fact, in 2015, 66% of all rotator cuff surgeries (48,568 of 74,120 cases) were conducted in hospitals with 30−100 beds.
In terms of the component ratio of procedure codes in accordance with hospital size, the proportion of isolated acromioplasty procedures (N0935) was higher in hospitals with 30−100 beds and clinics than in tertiary hospitals and general hospitals. Although it is difficult to pinpoint the exact cause of this phenomenon, it is possible that it may be a result of the differences in patients' disease severity or surgeons' surgical indications in accordance with hospital size. This result could be interpreted as indicating that small hospitals and clinics tend to perform isolated acromioplasty more aggressively as a treatment for impingement syndrome (5). The popularity of acromioplasty has rapidly increased recently in the United States as well as in the United Kingdom (57), and also accounts for approximately 30% of all surgeries for rotator cuff disease in Korea (Fig. 6). However, as evidence supporting the effectiveness of acromioplasty is unclear, and some reports show that it may be no more beneficial than physiotherapy (71527). Well-designed clinical trials are required to establish optimal indications for this procedure.
Despite the fact that this study employed a large sample size based on a nationwide database, it also has some limitations. First, there is a lack of detailed clinical data. It was difficult to identify symptom duration and whether conservative treatment was performed, as well as the duration of treatment prior to surgical treatment. Hence, this study could not accurately examine surgeons' preference for surgical treatment. Second, there was a change of procedure code during the period of this study. A new complex RCR code (N0938) was added after July 2014, so code N0938 was weighted lower than other procedure codes (Fig. 6). Third, we could not identify whether patients who received RCR (N0936–N0938) also received acromioplasty. Fourth, even patients who were converted to open surgery from arthroscopic surgery are classified as arthroscopic surgery cases because arthroscopic devices costs (N0031003) are still claimed. But, these patients may be quite small. Finally, there is a possibility of some code error in a large database.
The findings of this study revealed that age-adjusted rate of rotator cuff surgery per 100,000 persons rapidly increased between 2007 and 2012 in Korea, and that most rotator cuff surgeries are performed arthroscopically. Hospitals with 30−100 inpatient beds demonstrated the highest increase in rotator cuff surgeries, underscoring the fact that rotator cuff surgery is a popular procedure performed commonly even in small hospitals. However, there were varying component ratios of procedure codes depending on hospital size, with the proportion of isolated acromioplasty procedures higher in hospitals or clinics with less than 100 inpatient beds.
 XML Download
XML Download