

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus (DM) is a strong risk factor for coronary artery disease (12). Previous prospective studies have shown that patients with DM have a 2-fold increased risk of developing coronary artery disease (3), and 2 to 4 times higher risk of mortality caused by coronary artery disease (34). Patients with DM comprised approximately 30% of patients who underwent percutaneous coronary intervention (PCI) in the era of drug-eluting stents (DESs) (5). Post-PCI clinical outcomes were worse in patients with DM than in those without DM (6). In daily clinical practice, new-onset DM in some DES-treated patients is often encountered during long-term follow-up after PCI. Although the etiologies of DM are diverse, metabolic derangements maybe related with development of new-onset DM (7). Intensive lipid-lowering therapy might also contribute to occurrence of new-onset DM (8). There have been multiple studies regarding post-PCI clinical outcomes in patients with previously known DM. However, data regarding the incidence, predictors, and long-term clinical outcomes of new-onset DM in patients who underwent PCI, particularly DES implantation, are insufficient. Therefore, we sought to investigate the incidence, predictors, and long-term clinical outcomes of new-onset DM in DES-treated patients.
MATERIALS AND METHODS
Study population
Between July 2007 and December 2011, 6,777 consecutive patients received DES implantation. Among those patients, 729 patients were excluded from this analysis due to the following reasons: loss of follow-up or follow-up duration less than 1 year (n = 58), incomplete medical records with missing data on fasting plasma glucose or hemoglobin A1C (HbA1C) (n = 124), expected survival less than 1 year (n = 79), emergent PCI with hemodynamic compromise (n = 75), use of steroid medications (n = 18), renal dialysis (n = 62), major non-cardiac surgery within 3 months following DES implantation (n = 60), and prediabetes (n = 253) according to impaired fasting glucose and glucose tolerance. Because prediabetes could be a strong confounder, it was excluded from analysis in this study. Ultimately, 6,048 patients were enrolled. PCI procedures with DES implantation were performed according to current standard techniques (9). At least 12 hours prior to DES implantation, all patients received loading doses of aspirin (100 mg) and clopidogrel (300 mg). However, if this loading dose of clopidogrel was not administered, the patient instead received a 600 mg loading dose in the catheterization laboratory immediately prior to PCI. Unfractionated heparin was administered to maintain an activated clotting time longer than 250 seconds. Glycoprotein IIb/IIIa inhibitors were used at the operator's discretion. Post-procedure treatment included a 12-month prescription for dual antiplatelet therapy with 100 mg of aspirin and 75 mg of clopidogrel daily. The intensity of lipid-lowering therapy with statin was classified according to American College of Cardiology and American Heart Association guidelines (10).
Definitions of DM and study end-point
Each patient's diabetic status was determined using medical records and baseline laboratory data at the index procedures, and was defined in accordance with criteria from the American Diabetes Association (11). Because an oral glucose tolerance test was not performed in all patients, the laboratory diagnosis was made with fasting plasma glucose or glycated hemoglobin (HbA1c) levels. Patients who had previous history of DM, abnormal laboratory results (fasting plasma glucose > 126 mg/dL or HbA1c > 6.5%), or were already receiving DM treatment (such as oral hypoglycemic agents or insulin) at the index procedure, were assigned to the known DM group. Patients without previous history of DM and abnormal laboratory findings suggestive of DM at the index procedure were divided into two groups: non-DM group without occurrence of DM during follow-up and new-onset DM group with occurrence of DM during follow-up. If the patient without previous history of DM showed abnormal laboratory findings suggestive of DM during follow-up, a second laboratory test was recommended for the confirmation. After DM diagnosis, patients were usually treated with metformin in combination with lifestyle changes and continuing timely augmentation of therapy with additional agents to achieve and maintain HbA1c < 7.0% according to the American Diabetes Association guideline (11).
Major adverse cardiac event (MACE) was a composite of cardiovascular death, myocardial infarction (MI), stent thrombosis, or any revascularization. Clinical events were defined using criteria from the Academic Research Consortium (12). All deaths were considered cardiac deaths unless a definite non-cardiac cause could be established. During follow-up after hospital discharge, MI was defined as the presence of consistent clinical symptoms, electrocardiographic changes, or abnormal imaging findings, combined with a creatine kinase myocardial band fraction increase greater than the upper normal limit or an increase in troponin-T/troponin-I to > 99th percentile of the upper normal limit (1213). Definite, probable, and possible stent thrombosis was defined using Academic Research Consortium recommendations (1213). Any revascularization was defined as a PCI or bypass surgery of the DES-treated or de novo lesions. Revascularization was usually performed when clinically indicated (angiography shows diameter stenosis ≥ 50% by quantitative coronary angiographic analysis with ischemic symptoms or positive stress test results, or diameter stenosis ≥ 70% without ischemic symptoms or positive stress test results) (12).
Statistical analysis
Continuous variables were described as mean (± standard deviation [SD]) or median (interquartile ranges) values. Intergroup comparisons (new-onset DM group vs. non-DM group or known DM group) for continuous variables were performed using Student's t-test. Categorical variables were expressed as number (%) and the χ2 test was performed for intergroup comparison. Univariate and multivariate Cox proportional hazard regression analyses were performed to identify the independent predictors of new-onset DM, and to compare the risk of clinical events between the groups. Variables with P values < 0.5 from univariate analyses and clinically important variables were included in multivariate analyses. The cumulative rates of MACE in each group were obtained using Kaplan-Meier plots and compared using the log-rank test. Patients who were lost to follow-up were assessed at the time they were last known to be event-free. A P value < 0.05 was considered statistically significant. All analyses were performed using SPSS® Statistics 21 software (IBM®, Armonk, NY, USA).
RESULTS
A total of 2,365 patients were in the known DM group, accounting for 39.1% of the total study group. During the follow-up period, 436 (11.8%) of the 3,683 non-DM patients were newly diagnosed with DM at 3.4 ± 1.9 years after DES implantation and subsequently included in the new-onset DM group. The remaining 3,247 patients were assigned to the non-DM group. Fig. 1 shows patients flow. Baseline characteristics of these 3 groups (non-DM, new-onset DM, and known DM) are shown in Table 1. Compared with the non-DM group, the new-onset DM group had higher body mass index (BMI), higher serum triglycerides or fasting glucose level, and higher frequency of high-intensity statin therapy. In addition, compared to the known DM group, the new-onset DM group was younger, had higher BMI, higher ejection fraction, higher serum low-density lipoprotein cholesterol level, lower serum fasting glucose or creatinine level, lower frequencies of hypertension or multi-vessel disease, and higher frequency of high-intensity statin therapy.
Fig. 1
Patients flow.
DES = drug-eluting stent, PCI = percutaneous coronary intervention, DM = diabetes mellitus.
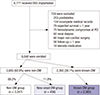
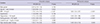
Table 1
Baseline characteristic among three groups categorized by diabetic status

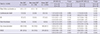
Predictors of new-onset DM were determined based on data from patients without DM at index procedure (n = 3,683 excluding 2,365 known DM patients). As shown in Table 2, univariate analysis revealed that high BMI, high serum triglycerides level, high serum fasting glucose level, and high-intensity statin therapy were associated with an increased risk of new-onset DM. In the multivariate analysis, all of these variables were also shown to be independent predictors of new-onset DM.
Table 2
Univariate and multivariate analysis of predictors for new-onset DM
Mean follow-up duration in this study was 4.0 ± 2.1 years in overall patients. The risks (hazard ratio [HR]) for clinical events during the follow-up period after DES implantation were calculated between the groups using the Cox proportional regression analysis (Table 3). Two separate analyses were performed between new-onset DM group vs. non-DM group and new-onset DM group vs. known DM group. Compared to the non-DM group, the new-onset DM group showed similar risks for an individual cardiovascular event and MACE. However, when compared to the known DM group, the new-onset DM group showed lower risk for MI, any revascularization, and MACE. After being adjusted with various clinical and procedural characteristics, the new-onset DM group still showed lower risk for MACE, compared to the known DM group (HR, 0.71; 95% confidence interval [CI], 0.51–0.99, P = 0.045). Fig. 2 shows the cumulative rate of MACE in the 3 groups by the Kaplan-Meier method. The 8-year cumulative rate of MACE was 19.5% in the new-onset DM group, which was similar to the cumulative rate (20.5%) in the non-DM group (P = 0.467), but lower than the rate (25.0%) in the known DM group (P = 0.003).
Table 3
Cardiovascular event rate and HR according to diabetic status and comparison with new-onset DM*
MACE was a composite of cardiovascular death, MI, stent thrombosis, or any revascularization.
HR = hazard ratio, DM = diabetes mellitus, CI = confidence interval, MI = myocardial infarction, MACE = major adverse cardiac event, BMI = body mass index.
*Data are expressed as number of patients (8-year cumulative event rates). †Adjusted with gender, age, BMI, hypertension, triglycerides level, creatinine level, ejection fraction, acute coronary syndrome, multivessel disease, stent number, stent diameter, and total stent length.
Fig. 2
Kaplan-Meier survival curves for MACEs. Estimated 8-year cumulative rates of MACEs (composite of cardiovascular death, MI, stent thrombosis, or any revascularization) were 19.5% in the new-onset DM group, 20.5% in the non-DM group, and 25.0% in the known DM group.
MACE = Major adverse cardiac event, MI = myocardial infarction, DM = diabetes mellitus.

DISCUSSION
The main findings of the present study are as follows: 1) in non-DM patients, the incidence of new-onset DM was 11.8% during the follow-up period after DES implantation; 2) the predictors of new-onset DM after DES implantation include high-intensity statin therapy, high BMI, and high level of fasting triglycerides and glucose; and 3) patients with new-onset DM after DES implantation showed similar clinical outcomes compared to non-DM patients, and better clinical outcomes compared with known DM patients. Although evidence from multiple studies have indicated that DM is a strong risk factor for coronary artery disease and DM patients show worse clinical outcomes after PCI, the data regarding new-onset DM after DES implantation has been limited. Results from this study provide new data on the incidence, predictors, and clinical outcomes of new-onset DM in DES-treated patients in real-world clinical practice.
In previous statin trials involving patients with stable coronary artery disease or stroke/transient ischemic attack, the incidence of new-onset DM was 6.1%–9.2% (1415). Furthermore, in patients without coronary artery disease, the incidence of new-onset DM was as low as 2.3%–3.0% (1617). In the present study, the incidence of new-onset DM was 11.8% in patients with DES implantation. Compared to previous studies, the higher incidence of new-onset DM in this study may be explained that the present study exclusively enrolled patients with severe coronary artery disease, which is sufficient to require DES implantation. Of course, these patients may have higher frequencies of obesity, hypertension, and abnormal serum glucose or lipid profile, all of which are well-known predisposing factors of DM as well as coronary artery disease (7).
Similar to results from previous studies (18), identified predictors of new-onset DM in this study included high BMI, high serum triglycerides, or high fasting glucose level. These factors are the main components of metabolic syndrome (19) with insulin resistance and endothelial dysfunction, which are the precursors of DM (72021). Also, high-intensity statin therapy was identified as a predictor of new-onset DM after DES implantation. Statins have been widely used for the primary and secondary prevention of cardiovascular diseases and play a major role in preventing the long-term vascular events in patients with DM (22). However, there have been several reports that statins may have diabetogenic potential (81618). According to the meta-analysis, this adverse effect is statin dose-dependent (23). Several possible mechanisms for the diabetogenic potential of statins have been suggested, including the finding that statins have been shown to inhibit glucose-induced Ca2+ signaling and insulin secretion by blocking Ca2+ channels in β-cells (24). In clinical practice, the majority of DES-treated patients received statin therapy for the secondary prevention of adverse cardiovascular events. In the present study, almost all (96%) study patients received statin therapy after DES implantation and 7% were prescribed high-intensity statin therapy. The current guidelines recommend high-intensity statin therapy in high-risk patients because more intensive statin therapy more effectively decreases cardiovascular events (14). However, when prescribing high-intensity statin therapy to non-DM patients after DES implantation, watchful follow-up for occurrence of new-onset DM may be warranted, especially in patients with some traits of metabolic syndrome such as high BMI, serum triglycerides, or fasting glucose level.
In the current era of DES, data for long-term clinical outcomes of new-onset DM in patients who underwent DES implantation are limited. In the present study, patients with new-onset DM after DES implantation showed similar clinical outcomes compared to non-DM patients, and better clinical outcomes compared with known DM patients. When compared to the known DM group, the new-onset DM group had a lower risk of MI, any revascularization, and MACE. Of note, new-onset DM may have negative effects on patient outcomes in the future. However, as shown in the present study, the 8-year cumulative rate of MACE in the new-onset DM group was not inferior to that in the non-DM group. Although not presented in the Results section, the 8-year cumulative rate of MACE in patients with prediabetes (n = 253, who were excluded from this study) was 18.4%, which was also similar with the rate of MACE in the new-onset DM group (P = 0.417). Taking all the results of the present study into consideration, physicians should keep patients with severe coronary artery disease requiring DES implantation under constant vigilance, particularly if patients have features of metabolic syndrome. However, physicians should not hesitate to prescribe high-intensity statins on account of their potential diabetogenic effects, because of the high benefits that statins have on the outcomes of cardiovascular disease by modifying metabolic derangement. Based on results from a previous primary prevention study, the cardiovascular and mortality benefits of statin therapy exceed the risks from new-onset DM (25). Therefore, even though patients may be diagnosed with new-onset DM after DES implantation, we expect that their clinical outcomes may not be worse compared to those of non-DM patients, and may even be better than those of known DM patients.
This study had several limitations. First, this analysis was a retrospective study. Second, fasting plasma glucose and HbA1C levels were the only serologic markers used to assess DM status. If regular check-ups with an oral glucose tolerance test were performed during the follow-up period, the number of patients diagnosed with new-onset DM may have differed. Third, although a second laboratory test was recommended for the confirmation if the patient without previous history of DM showed abnormal laboratory findings suggestive of DM, not all patients underwent the second test. Fourth, we could not collect data on some markers of metabolic syndrome including abdominal circumstance. Fifth, patients' vital status was not validated using the national data.
In conclusion, the incidence of new-onset DM was 11.8% in non-DM patients during the follow-up period after DES implantation. Predictors of new-onset DM after DES implantation included high-intensity statin therapy, high BMI, and high serum triglycerides or fasting glucose level. Patients with new-onset DM after DES implantation showed similar clinical outcomes compared to non-DM patients, and better clinical outcomes compared with known DM patients.
 XML Download
XML Download