

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease is a leading cause of morbidity and mortality globally [1]. Cardiac Rehabilitation (CR) that is based on exercise plays a role in reducing cardiovascular- related mortality, all-cause mortality, and rehospitalization, as well as improving the patient's quality of life [234].
In the United States, despite the benefits of CR, the average participation rate is only 14% in patients who are admitted to the hospital for acute Myocardial Infarction (MI) and 31% in patients who had coronary artery bypass graft surgery [5]. Additionally, the CR participation rate remains suboptimal in the United Kingdom and Canada; the rate ranges from only 20% to 30%[6].
Some factors that are known to interrupt patient participation in CR include older age, female sex, lack of recommendation from physicians, lack of patient's and physician's awareness of CR programs and their benefits, insufficient insurance coverage, lack of family support, low socioeconomic status, lack of vehicle and driving abilities, occupational problems, decreased motivation, and lack of self-efficacy [7891011].
A low referral rate was one of the main reasons for the interruption of enrollment in CR programs [12]. Other studies have effectively attempted to increase CR enrollment by approximately 1.6~2.6 times using an automatic referral system and patient-physician (liaison-facilitated) discussion [1213]. In another study, to improve participation in CR, CR liaison nurses were added to the rehabilitation protocol. The CR liaison nurse recruited patients to attend a CR program, supported the patients regularly by providing advice and information on CR and secondary prevention of MI over the telephone, arranged patient's first follow-up appointment for CR, and discussed with the patient during their follow-up visit to the hospital after discharge. CR liaison nurses have been involved throughout the CR program, and the CR participation rate increased to 40%, compared with 10% in a control group [14].
Previous studies have shown that the longer the patient waits for CR, the lower the eventual participation rate. The participation rate decreased by 1% for every 1-day increment in wait time until the first CR program after discharge [1516].
Moreover, the home-based CR was associated with higher participation rates [17]. Previously conducted meta-analyses have shown that home-based CR increased CR participation rates by more than 4%, and home-based CR was proven to be cost-effective [18].
Our medical center established a Clinical Pathway (CP) to increase the CR participation rate in patients with MI who underwent Percutaneous Coronary Intervention (PCI) including an automated referral system. However, the rate of CR participation was as low as 20~30%.
To increase this low CR participation rate, we revised the CP of CR in April 2016. The CP was revised mainly to reduce the number of hospital visits and CR wait time and to reinforce the role of the CR liaison nurse. Hence, the purpose of this study was to investigate the effect of the revised CP on CR participation rate at 1 month and maintenance rate at 3 months on patients with MI.
METHODS
1. Study Design
This is a retrospective study to investigate the effect of CP revision on CR participation rates.
2. Setting and Samples
A total of 258 patients with MI were admitted to our hospital, which was a Chungbuk National University hospital in Chungcheongbuk-do, and underwent PCI from July 1, 2015, to December 31, 2016. Of these patients, 250 were referred by a cardiologist, with the exception of 8 patients (4 who died from MI, 2 who absconded, and 2 with insufficient chart data).
Starting from April 1, 2016, the CP for CR after PCI in patients with acute MI was changed from an automatic referral system between the Division of Cardiology and CR center to a revised CP with an additional intervention. Based on the revised CP, the study periods were divided into two, namely, July 2015 to March 2016 and April 2016 to December 2016, each of which was 9 months long. A total of 110 patients from the previous CP and 140 from the revised CP were referred.
Among the 250 patients who were included in the CR CP, 51 were excluded based on the absolute and relative contraindications (e.g., ongoing unstable angina, decompensated heart failure, acute pulmonary embolism, deep vein thrombosis, physical disability that precludes safe and adequate testing, etc.) to exercise testing of the American Heart Association's guidelines [4]. Finally, a total of 199 patients were eligible for CR.
3. Protocol and Procedure
1) Common protocol in previous and revised CP
The patient was admitted to the hospital after PCI due to MI. The average length of hospital stay was 3 days. In the hospitalization period, a dietitian gave the patient healthy eating advice, and the patient was assessed psychosocially.
An automated referral system has been in operation since 2009 from the Division of Cardiology to the cardiac rehabilitation center on the first day of admission. Thereafter, a physiatrist examined the patient to assess his or her eligibility for CR and introduced the CR program accordingly. The CR liaison nurse explained the overall CR process, its effect, and risk modification methods for the secondary prevention of cardiovascular disease.
2) Previous CP protocol
After discharge, the patients visited the cardiology outpatient clinic to be prescribed medication and have their medical condition checked 2 weeks post-discharge. At 1 month post-discharge, the patients underwent a Cardio- Pulmonary Exercise test (CPX) and body composition analysis at their desired date. Within 1 week after CPX, the patient made a third visit appointment. The physiatrist explained the results of the CPX test and recommended participating in CR on the third visit.
Based on the CPX test results, the patients were divided into low-, middle-, and high-risk groups according to the risk classification guidelines of the American Association of Cardiovascular and Pulmonary Rehabilitation [19]. All participants underwent an electrocardiogram-monitored CR exercise program for 8 weeks. After 8 weeks, participants were administered a CPX test to evaluate the effects of the CR program.
3) Revised CP protocol
The revised CP was designed to reduce the number of times the patient visited the hospital and the waiting time before starting CR. It was also designed to strengthen the role of the CR liaison nurse. In addition to the role of the previous CP, the CR liaison nurse coordinated the outpatient clinic's schedule and that of CPX testing and called the patient the day before the hospital visit to encourage patient to come to the CR center. The CR liaison nurse provided re-education about CR and risk factor modification at the first cardiology outpatient clinic visit after discharge. After the first CPX test, the CR liaison nurse sent a text message to the patient every week to encourage him or her to exercise and provided information on the modification of cardiac risk factors.
We set up a reservation system for the CPX test and CR center on the same day the patient visited the hospital for the first cardiology treatment 2 or 3 weeks post-discharge. To change the reservation system for the revised CP, cardiologists and physiatrist consulted with one another. After the change in the reservation system was decided, the physiatrist explained the revised CP contents to the CR liaison nurse in the entire cardiac ward and related medical personnel. To determine the feasibility of the CPX test, we measured the patient's pulmonary function test, gait speed, grip strength, and body composition on the day of discharge, or one day prior to discharge.
After discharge, the patient was accompanied to the CPX and cardiac rehabilitation center on the day of visiting the cardiology outpatient clinic for medical checkup. On the same day, patients participated in the CR program. This reduced the number of hospital visits and the waiting times for CR.
The home-based CR program was provided to all patients in the low-risk group and some in the moderate-risk group who were restricted to visiting the hospital periodically because of work or other reasons stated in the revised CP. In the revised CP, a cardiac exercise diary was also created and distributed to these home-based CR patients.
A physiatrist prescribes CR regimens about the exercise frequency, intensity, time, and type that were based on CPX results and their previous exercise status or activities. The patients manually recorded their daily exercise routine, including the exercise type, intensity, time, and side effects in a cardiac exercise diary. After the home-based CR regimen was performed for 8 weeks, the patients visited the CR center to undergo CPX testing. The hospital-based CR program was recommended to all patients in the high-risk group and some in the moderate-risk group. Patients who wanted to participate in the hospital-based CR program underwent the program for 8 weeks.
4. Ethical Considerations
This retrospective medical chart review study was approved by the Institutional Review Board of Chungbuk National University Hospital (IRB No. 2017-06-014).
5. Statistical Analysis
Between-group differences were tested using Pearson's χ2 or Fisher's exact test for non-continuous variables such as gender, age subgroup, diagnosis, hypertension, diabetes mellitus, hyperlipidemia, current smoking status, participation rate, maintenance rate, risk groups, subgroup of ejection fraction, metabolic equivalents, use of beta-blocker, and cardiac events.
An independent t-test was used to statistically analyze age, ejection fraction from an echocardiogram, VO2max, systolic blood pressure, diastolic blood pressure, body mass index, number of involved vessels, number of inserted stents, number of hospital visit, and the waiting days for CR of patients who underwent CPX at 1 month in the previous CP and revised CP groups.
The Mann-Whitney test was used to analyze age, ejection fraction from an echocardiogram, VO2max, systolic blood pressure, diastolic blood pressure, body mass index of patients who underwent CPX at 3 months in both groups.
All statistical analyses were performed using the SPSS/WIN 24.0 software (IBM SPSS Software; IBM Corp, Armonk, NY), with a statistical significance level of p<.05
RESULTS
1. General Characteristics of the Eligible Patients for CR in Both Groups
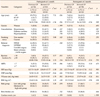
In previous CP, 92 patients (73 men and 19 women) were included. In the revised CP, 107 patients (84 men and 23 women) were included. The patients were significantly older in the revised CP (t=−2.14, p=.034). The percentage of patients with diabetes was significantly lower (χ2=4.40, p=.036) and patients with smoking habits were significantly higher in the revised CP (χ2=6.94, p=.031). There was no significant difference in other general baseline characteristics (Table 1).
2. Characteristics of Patients Who Participated in the CR at 1 month and Maintained for 3 months after Undergoing PCI
The characteristics of participants at 1 month CPX before and after CP revision are as follows. In the revised CP group, significantly more patients were over 60 years old than in the previous CP group (χ2=7.31, p=.026). In addition, as a result of CPX, there is a tendency for an increased number of moderate- to high-risk patients in the revised CP group (χ2=3.28, p=.070). The percentage of patients with a lower ejection fraction (less than 50%, χ2=3.77, p=.052) and an exercise capacity less than 7 metabolic equivalents (χ2=2.95, p=.086) tended to be higher in the revised CP group than in the previous CP group.
There were no differences between the two groups in terms of beta blocker (p=.742) use that could affect CPX or the rate of cardiac events during CR program (rehospitalization or visiting the emergency room because of cardiac symptoms such as chest pain). There was no significant difference in other characteristics of CR participants at 1 month. Although not shown in the table, there was no difference between the two groups in terms of the number of affected blood vessels (1.75±0.74 versus 1.92±0.87 in previous and revised CP, t=−0.87, p=.390) and the number of stents of PCI (1.29±0.75 versus 1.25±0.79, t=0.24, p=.808).
Each one patient in both groups was readmitted and two patients in the revised CP group went to the emergency room due to chest pain, but were discharged without any problems. Three of the revised CP group with cardiac events participated in CPX at 3 months. There was no significant difference in the characteristics of patients who underwent a 3-month CPX in both groups (Table 2).
3. Participation and Maintenance Rates of CR in Both Groups
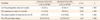
Of the 92 patients in the previous CP group, 24 (26.1%) participated in a 1-month CPX program and 11 (12.0%) patients were maintained in a 3-month CPX program. Of the 107 patients in the revised CP group, 65 (60.7%) participated in a 1-month CPX testing program and 38 (35.5%) patients were maintained in a 3-month CPX testing program. The participation rates at 1 month (χ2=24.04, p< .001) and maintenance rates at 3 months (χ2=11.49, p<.001) increased significantly after the CP was revised (Table 3).
4. Change in the Mean Number of Hospital Visits to Participate in CR and the Mean CR Wait Times for the First CPX Test
The mean number of hospital visits for CR participation was 3.50±0.83 times in the previous CP group versus 1.91±0.86 times in the revised CP group (t=7.92, p<.001). The mean number of times it took the patient to visit the hospital to complete the CR program significantly reduced after the CP was revised.
The average number of days the patient waited for the first CPX test was 43.42±17.64 in the previous CP group versus 26.29±10.57 in the revised CP group (t=4.47, p< .001). The CR wait times significantly reduced after the CP was revised (Table 3).
DISCUSSION
To increase the rate of participation in CR, we revised the CP using a multifaceted approach by reducing the number of hospital visits and CR wait time and reinforcing the role of the CR liaison nurse. This led to a significant increase in the CR participation rates (approximately 2.3 times greater than before) and maintenance rate of CR. This indicates a tendency that CP revision is effective especially on elderly and high-risk patients. Even without additional equipment and facilities, the personalized simplified CR program, including the home-based program and weekly text message, was effective.
In the previous CP group, patients performed the first CPX test at 4 weeks post-discharge due to patient's condition and medical safety according to the Canadian Cardiovascular Society guidelines on CR wait times published in 2006. They recommended that a 30-day CR wait time was preferable [20]. However, in later studies, as the CR wait times increased, the CR participation rate decreased [1516]. Several other studies have shown that reducing the CR wait times increased CR participation rates and does not increase complication rates (such as mortality, cardiac event, physical ability etc.) [212223]. Based on the above and recent Japan's guideline [24], we reduced the CR wait times and the number of hospital visits by performing CPX in accordance with the first cardiac outpatient clinic day at 2 or 3 weeks after discharge. The CR wait time was reduced by approximately 17 days (39%) after CP revision. We also found that reducing CR wait times was innocuous because there were no differences in the rate of cardiac events (rehospitalization or visiting the emergency room because of cardiac symptoms such as chest pain).
Busy social work, transportation problems to the hospital, and cost are the main factors impeding CR participation [91011]. Thus, a decrease in the number of hospital visits could be beneficial in terms of job conflicts, busy schedules, and cost. The previous CP group was required to come separately from the cardiology outpatient clinic and CR center. At that time, to increase the CR participation rate, we performed the CPX test on the patient's desired date. Conversely, there were many inconsistencies between the CPX testing and CR center dates. The patient needed to come to the CR center once more to participate in the CR program. After CP revision, the number of hospital visits also reduced by approximately 1.6 times with decreasing CR wait times. Our study's initial goal was to reduce the number of hospital visits by one; however, patients are required to undergo blood testing before coming to the hospital, or they may present with other medical conditions. Therefore, there were actually more hospital visits than expected, both before and after the CP was revised.
A home-based CR program was also added to the revised CP. It is known that home-based CR programs have a similar effect on physical ability, mortality, morbidity, and quality of life to existing medical center-based CR programs [2526]. Additionally, home-based CR was known to increase CR participation rates by approximately 4~16% and reduce the costs of CR. In the previous CP, all participants in the CR visited the hospital once or twice a week and underwent CR exercise for 30 minutes by physician's supervision. In the revised CP, a home-based CR was provided primarily for low-risk patients and the patients recorded self-exercise for 8 weeks. For a home-based CR, patients were given a more detailed explanation of CPX results and future exercise plan. The patients were informed of the target heart rate for exercise and subjective exercise intensity using the Borg Rating of Perceived Exertion Scale.
The exercise diary was produced according to the American Heart Association's guidelines [4]. In this diary, various exercises according to the level of metabolic equivalent were presented, and the patients were informed of the exercise prescription including the kind of exercise, frequency, time, and intensity. In addition, the type, time, and intensity of exercise performed by patients for 8 weeks could be recorded. It was also possible to record the heart rate, blood pressure, and occurrence of chest pain during exercise. If the patient doses not have monitoring equipment such as a wrist watch with a heart rate monitor, he could record subjective exercise intensity by Borg Rating of Perceived Exertion Scale. To promote home-based CR, we distributed exercise diary and sent weekly text messages to the patients.
The intervention effect by the CR liaison nurse on CR through recruitment, education, and follow-up of patients was proven [27]. Our CR liaison nurse also provided patients with additional face-to-face education on the CR program, telephone calls to encourage participation, and text messages for self-exercise and secondary prevention. This would have had a positive impact on participation and maintenance of CR.
In a Chinese study, a nurse-led CR program was performed on patients with angina pectoris or myocardial infarction. It has been proven effective in improving the health behaviors and reducing cardiovascular risk factors. The study consisted of two phases. In phase 1, an experienced cardiac nurse educated the patient and caregivers in seven topics (self-management principle, medication management, angina prevention, physical exercise, dietary management, smoking cessation, and family support). In phase 2, the experienced cardiac nurse instructed the patient and caregivers to perform seven topics that were previously taught during 12 weeks of cardiac rehabilitation, either by visiting or telephone call [28]. It was able to exert positive influence on the patient's participation and outcome through active nursing intervention beyond the existing routine care. In CR, nurses are expected to play an important role in patient education and participation in treatment.
Old age and lower physical functioning were two of the main barriers to CR participation [78]. In the recruitment phase, the average age of patients in the revised CP group was higher than that in the revised CP group. This could have an adverse effect on increasing CR participation rates in the revised CP group; nonetheless, the revision of the CP created a 2.3 times improvement of the participation rate. In the previous CP group, the higher percentage of diabetic patients is a factor that can lower the participation rate [7], but a lower percentage of smokers is a factor that can increase the participation rate [11]. It is not known exactly how these factors affected CR participation rate in the previous CP group. The positive and negative factors for the participation rate exist simultaneously, which is not a big problem in interpreting the result with 2.3 times increased participation rate. However, this is a limitation of our retrospective study.
This study has several limitations that should be acknowledged. First, this study was retrospectively designed. Data on barriers to CR participation were limited, further limiting our analysis of compounding factors. Second, the low number of participants did not allow us to statistically verify changes in the participation and compliance rates among women, who are known to have low referral and participation rates. Third, because of the multidirectional approach that was used, we could not analyze the effects of one-on-one intervention. It was difficult to evaluate which exact part of the revised CP was effective. Fourth, we did not consider seasonal changes in CR participation rates. Patients may not be able to participate in CR in very cold seasons such as January and February. Fifth, we limited our study to patients with MI who received PCI. Those who had coronary artery bypass surgery, heart failure, heart valve replacement, and other CR indications were not included. Further research involving more patients is required to determine whether the changes in the CP affect the compliance and maintenance rates of the CR program, mortality, and patient's quality of life. A further study is needed to evaluate long-term participation rates for more than 6 months.
CONCLUSION
This retrospective study demonstrates that the revision of CP can increase CR participation rates. This CP revision was made to reduce the mean number of hospital visits for CR and the CR wait times, strengthening the role of the CR liaison nurse in patient's education and follow-up and adding the home-based CR program. This suggests that even though patient factors have not changed, the efforts of the medical team can increased the participation rate in CR.
Given the necessity and importance of CR, it is essential to increase CR participation rates. For this, CP revision in terms of inter-physician communication for efficient CP and additional nursing interventions for patient recruitment, education, and follow-up should be considered.



 XML Download
XML Download