

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The horseshoe kidney is one of the most common anatomical variations of the kidney with an incidence of one in every 600-800 individuals (1, 2), and is twice as commonly in males (3). It results from anomalous fusion at the lower poles (95% of cases) or at the upper poles. The horseshoe kidneys vary widely in origin, number, and size of the renal arteries and veins. Comorbidities include ectopic ureterocele, vesicoureteral reflux, ureteropelvic junction (UPJ) obstruction, polycystic kidney disease (PCKD) and ureter stone (4). The horseshoe kidney transplantation is associated with a higher percentage of primary non-function because of thrombosis of the vessels (5). Although these features make transplantation more difficult technically, it is not impossible to transplant the horseshoe kidney. In addition, it could be a good solution for the shortage of organ donors. We report a case of transplantation of a split horseshoe kidney from a cadaveric donor. To the best of our knowledge, this is the first case reported in Korea.
CASE DISCRIPTION
A 34-yr-old female with a history of depression was admitted at March 30, 2013 after taking an overdose of antidepressant with alcohol. She was diagnosed as being brain dead. She had no known history of kidney or urinary tract disorders. Blood urea nitrogen was 5 mg/dL and creatinine 0.91 mg/dL. Blood type was O +. Preoperative ultrasound revealed normal parenchymal echogenicity. No abnormal focal lesion was found in any part of the kidneys. However, the ultrasound was not able to identify the shape of horseshoe kidney and its variant vasculature.
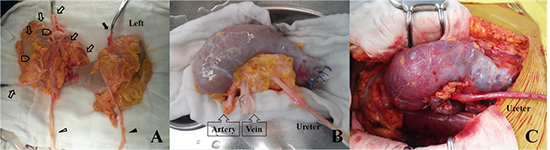
During organ harvest, the horseshoe kidney was identified. The isthmus was placed anterior to the aorta and the inferior vena cava. After harvesting the liver, en bloc nephrectomy was performed. In bench surgery, inspection revealed the left kidney having normal vasculature with single renal artery and vein, whereas the right kidney had numerous arteries and veins (Fig. 1A). The isthmus contained a broad band of normal parenchyma. The kidney did not have urinary collecting system variations or any other renal abnormalities. The kidney was divided at the midline of isthmus, preserving its vasculature and urinary collecting system. Intracorporeal suturing was used to repair the inner layer of the renal parenchyma with 3-0 polyglactin sutures for hemostasis. The edges of the renal remnant (outer layer) were approximated using 2-0 absorbable polyglactin sutures after inner layer renorrhaphy (Fig. 1B). The divided right kidney was discarded due to its numerous arteries and veins.
The recipient was a 31-yr-old female with end stage renal disease secondary to hypertension and Henoch-Schönlein purpura. She had been on hemodialysis using arteriovenous fistula for 4 yr. Blood type was O +. The divided left kidney was transplanted at the recipient's right iliac fossa. The renal artery was anastomosed to the recipient's right external iliac artery, and the renal vein anastomosed to the right external iliac vein, in an end-to-side fashion. After declamping, the kidney was well perfused and started clearing (Fig. 1C). Cold ischemia time was 7 hr. Urinary tract continuity was established by ureteroneocystostomy using Lich-Gregoir technique with a double J stent insertion.
Immunosuppressants were given according to a routine protocol. Doppler ultrasound showed well-perfused parenchyma. Resistive index was 0.72 (Fig. 2A). A technetium 99m-diethylene triamine pentaacetic acid (99mTc-DTPA) renal scan on postoperative day 7 was normal with no leak from the divided isthmus. The glomerular filtration ratio (GFR) of the transplanted kidney was 66.2 mL/min on postoperative day 7 and improved to 84.69 mL/min on postoperative day 14 (Fig. 2B). Creatinine dropped to 0.94 on the postoperative day 9. The recipient had an uneventful recovery (Fig. 2C, D). The transplanted kidney has been functioning well up to the point of this report (12 months after transplantation).
DISCUSSION
The classic features of the horseshoe kidney on a plain abdominal X-ray are low-lying position and location close to the vertebral column. It can have a vertical or outward axis with the lower poles being more medial than in the normal kidney (6). Ultrasound can detect the joining isthmus in the midline, but may not always be identified. In a previous analysis of 34 patients, 10 (29%) patients were diagnosed with horseshoe kidney in the initial sonogram. The others needed additional tools including excretory urography (n=20) or computed tomography (CT; n=14) for diagnosis (7). In our case, preoperative ultrasound showed normal parenchymal echogenicity. The ultrasound was not able to preoperatively identify the shape of the horseshoe kidney and its variant vasculature. During organ harvest, the horseshoe kidney was identified. En bloc nephrectomy was performed. Right kidney had numerous small arteries and veins that had developed in several directions. Several arteries did not arise from the aorta, and their origin was not identified. The right kidney was not suitable for en bloc transplantation. Fortunately, the left kidney had a single renal artery and vein. The kidney was divided at the midline of isthmus, preserving its vasculature and urinary collecting system. The edge of isthmus was sutured water-tight. A report from Europe described immediate discard of 27% kidneys and discard of 9.6% after division. The majority of discarded kidneys had complex vascular anatomy and urinary collecting system injury or had no suitable recipients (8).
Some procedures for a safe separation were introduced from previous reports. One is injecting methylene blue dye into the renal artery to identify the blood supply territory (9). At the time of separation, to reduce post operative parenchymal wound, cone-like excision of isthmus is recommended so that the wounded edge can be brought together. During organ harvest, to prevent from injury of vessels and urinary collecting system, en bloc extraction including the aorta and the inferior vena cava should be performed (10). In our case, close inspection was performed but contrast injection was not. The divided isthmus remained dark red in color and achieved hemostasis after declamping (Fig. 1C). Fortunately, the vascular supply of isthmus seemed to be dependent on the left kidney. We think it would have been better to inject the dye to identify the blood supply before separation.
There are some possible problems that interfere with the horseshoe kidney transplantation. The horseshoe kidney can show symptoms of urinary tract infection, vesicoureteral reflux, hydronephrosis, urine stasis, and nephrolithiasis. Also, comorbidities such as ectopic ureterocele, UPJ obstruction, and PCKD can occur (4). Close identification of asymptomatic problems and be able to cope with possible difficulties is essential. Another problem is that the incidence of Wilm's tumor in people who have the horseshoe kidneys is twice as high as in the general population. The isthmus tends to have an increased potential of carcinoma development (11, 12). No case has been reported, but it seems likely to be found in the future due to immunosuppressive therapies (2). In this respect, using mTOR inhibitors may be helpful; a low incidence of cancer in a meta-analysis of more than 30,000 renal transplant patients was reported (13).
Most importantly, the horseshoe kidneys vary in anatomy of renal vessels and ureteral anomalies. These features make them technically more challenging for transplantation. Despite the anatomical anomalies, the kidney is histologically normal and the graft functions well after transplantation. Previous studies showed that the transplantation of the horseshoe kidneys, either en bloc or split, produced the same results compared with the transplantation of kidneys with a normal anatomy (8, 9).
In conclusion, we report a successful case of split horseshoe kidney transplantation from a cadaveric donor. This is the first transplantation case of a horseshoe kidney reported in Korea. Although the horseshoe kidneys have the potential for anatomical variation, careful inspection, imaging, and knowing the exact anatomy of the kidney could lead to successful transplantation. Despite the fact that it requires a highly surgical technique, the horseshoe kidney is suitable for transplantation as it could be effective as a normal kidney and could also be a possible solution for organ shortage.


 XML Download
XML Download