

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Pilomatricoma is a benign cutaneous tumor which presents as solitary, slow-growing, firm nodule with normal overlying skin1. Exophytic pilomatricoma, an uncommon subtype, shows distinctive features such as rapid development, reddish exophytic appearance, surface alteration suggestive of perforation, and relatively shallow location1. Here we present a case of exophytic pilomatricoma which resembled keratoacanthoma.
An 89-year-old female patient visited dermatology clinic because 3-month-old mass on her glabella started to increase in size abruptly. The lesion was firm dome-shaped mass with brownish crust in the center. The peripheral area of the mass showed irregular mixture of erythematous and whitish color (Fig. 1). At initial visit the mass measured approximately 10 millimeters in diameter. The patient did not recall any history of trauma prior to lesion appearance. Under the impression of keratoacanthoma partial wedge biopsy was performed.
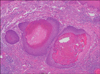
Upon histologic examination, instead of keratin-filled crater and epithelial proliferation the mass was surrounded by basaloid cells with eosinophilic ghost cells in the central portion. These findings led us to suspect pilomatricoma rather than keratoacanthoma. For further evaluation complete surgical excision was conducted. The resected tumor revealed multiple masses in dermis layer with histologic findings equivalent to the previous specimen (Fig. 2). Considering the visual appearance and the histologic features we diagnosed the mass as exophytic subtype of pilomatricoma.
Pilomatricoma is a common tumor especially among children but its accurate preoperative diagnosis is challenging due to clinical resemblance to various other tumors. In a study of 346 pilomatricomas by Pirouzmanesh et al.2 more than 70% of the cases were mistaken for 17 other tumors. Nevertheless, keratoacanthoma was not in the list of possible misdiagnosis. This finding suggests that clinical resemblance to keratoacanthoma is much more unusual. So far, it has been reported in only 2 cases34.
In some cases of exophytic pilomatricoma when elimination of the tumor content occur they are more often referred to as perforating pilomatricoma. This distinctive feature can accompany varying degrees of epidermal ulceration. When degree of ulceration is minimal the phenomenon is referred to as transepidermal elimination. As there are more than a dozen cases reported so far this subtype seems to be more common compared to exophytic pilomatricoma5.
Clinical features distinct from typical pilomatricoma include rapid growth and shallow location. These findings can also be found in cases of perforating pilomatricomas5. Due to rapid growth of the tumor clinicians have a shorter time to diagnosis5. This can be thought to contribute to the low incidence of both exophytic and perforating pilomatricoma.
The treatment of choice for pilomatricoma is surgical excision. Although some authors reported a successful treatment with shave biopsy, electrocautery, and curettage the recurrence rate with these methods has not been studied yet1. With surgical excision the recurrence rate is low. In one study average time to recurrence was 1.6 years, indicating the need for long term follow-up monitoring after the treatment2.

 XML Download
XML Download