

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Pigmented purpuric lichenoid dermatosis of Gougerot-Blum is an uncommon subtype of pigmented purpuric dermatosis (PPD). It is clinically characterised by tiny lichenoid papules that tend to fuse into plaques of various hues and are observed commonly on the legs but rarely on the trunk. It is morphologically characterised by but histopathologically indistinguishable from other entities of PPD1. Therefore, dermoscopy can be a highly valuable tool for accurate diagnosis2.
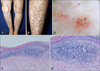
A 61-year-old woman presented with localized orange to brown lichenoid macules and papules on both legs for 3 years without any symptoms (Fig. 1A, B). Histopathological examination of the lichenoid papule revealed dense lichenoid cellular infiltration composed of lymphocytes, extravasated red blood cells, and hemosiderin in the upper dermis (Fig. 1C, D). Dermoscopy revealed round to oval red dots and globules with orange-to-brown-pigmented scaly patches (Fig. 1E).
PPD is a chronic and relapsing disorder characterised by a symmetrical rash of petechial and pigmentary macules usually confined to the lower limbs. PPD have been traditionally divided into the following six clinical entities: 1) progressive PPD (i.e., Schamberg's disease), 2) purpura annularis telangiectodes (i.e., Majocchi's disease), 3) lichen aureus, 4) PPD of Gougerot-Blum, 5) itching purpura, and 6) eczematid-like purpura of Doucas-Kapetanakis3. PPD of Gougerot-Blum is likely a variant of Majocchi's disease. It is diagnosed based on clinical and histopathologic features. However, PPD of Gougerot-Blum might clinically resemble Kaposi's sarcoma, mycosis fungoides, cutaneous vasculitis, and traumatic purpura. Dermoscopy is a non-invasive method that can be useful for making a correct diagnosis by differentiating coloured skin lesions. It complements clinical examination and allows improvement of the accuracy of diagnosis4.
To the best of our knowledge, dermoscopic findings in PPD of Gougerot-Blum have not been reported yet. There were only two reports24 of dermoscopic findings of PPD, lichen aureus. As published by authors, it exhibit a diffuse copper background, with red globules, plaques and round-to-oval dots, some gray dots and a network of interconnected pigmented lines.
In comparison, in the dermoscopic examination in the present case of PPD of Gougerot-Blum, small polygonal or round red dots and globules were observed underlying orange to brown scaly patches.
Vazquez-Lopez et al.5 suggested that dermoscopic patterns of purpuric lesions correlated to histopathologic findings. PPD are related to variable amounts of erythrocytes, lymphocytes, and siderophages surrounding swollen blood vessels within the upper part of the dermis, with or without epidermal changes. Therefore, the difference in the dermoscopic findings of lichen aureus and PPD of Gougerot-Blum is caused by the variable amounts of cell components.
In the present case, the orange to brown patches can be explained by the dermal infiltrate of lymphocytes and histiocytes, and by hemosiderin. Difference in the color of the background partially reflects the condition of extravasated erythrocytes. The red globules in our case can correspond to the histological finding of intact erythrocytes.
To conclude, dermoscopy could be a useful complement for a correct diagnosis of PPD of Gougerot-Blum, but further studies are required to generalize the dermoscopic findings in PPD of Gougerot-Blum described herein.
 XML Download
XML Download