

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatic hemangioma is a common non-epithelial neoplasm of the liver with a wide range of incidence, ranging from 1% to, 20%.1 It is usually asymptomatic and incidentally detected but prompts a flurry of investigations and lot of anxiety for the patient, because metastasis is the most common differential diagnosis.2 Though current recommendations are in favor of observation, even for large hemangiomas, the diagnostic dilemma leading to anxiety, coupled with symptomatology (related to pressure/capsular stretch), leads to consideration of surgery for these neoplasms. The surgical procedure of choice, whether enucleation or liver resection, is still debatable. Major hemodynamic changes can occur during surgery, especially massive blood loss. Postoperative complications, including bile leaks, have been reported to occur more frequently with liver resections than with enucleation.34
MATERIALS AND METHODS
We analyzed eighteen patients with hepatic hemangioma who were operated on from January 2011 to December 2016 at the Hepato-pancreato-biliary surgical unit of Tata Memorial Hospital. Preoperative demographic parameters, imaging findings, and indication for surgery were recorded. A detailed record of intraoperative parameters, such as operative time, intra-operative blood loss, and blood transfusions required, was maintained. Post-operative parameters, such as liver function tests on post-operative days 1, 3, and 7 (or earlier if clinically indicated) and postoperative hospital stay was noted. Postoperative complications were classified according to the Clavien Dindo (CD) grades.8 A survey of patient symptoms after operation was done by telephone 3 months after the date of surgery.
Data collection and statistical analysis were done using SPSS (ver. 21.0) and a Mann-Whitney test for continuous variables. A p value <0.05 was considered to be statistically significant. Spearman coefficient (rho) was used to correlate the size of the lesion with various intraopertaive and postoperative parameters to assess their bearing on surgical outcomes.
RESULTS
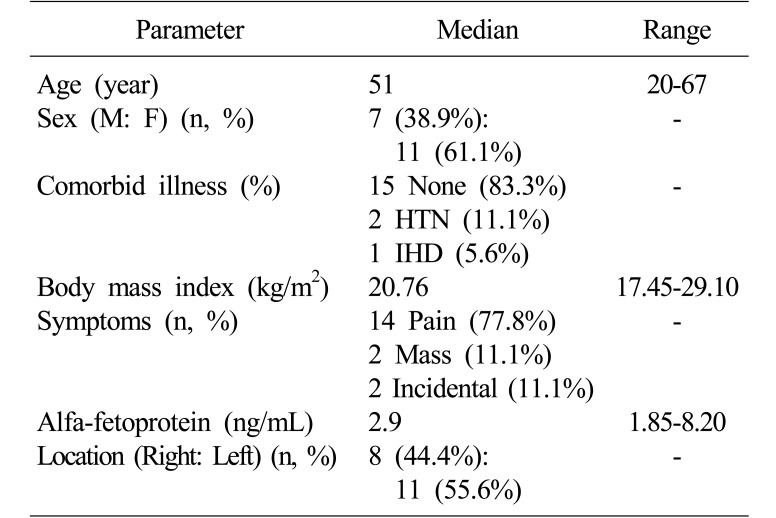
Of the 440 liver resections performed at Tata Memorial Hospital in the study period, 18 were done for suspected hemangiomas (4.09%). Basic demographic and clinical profiles of the patients are elaborated in Table 1. None of the patients had a background of cirrhosis on biochemical or radiological evaluation. All patients had a normal hematological evaluation, with no evidence of consumptive coagulopathy.
Six out of 18 (33.3%) patients had atypical imaging characteristics that led to diagnostic uncertainty. Of these 6 patients, 3 (16.7%) underwent a preoperative biopsy, 2 (11.1%) of which were inconclusive, whereas 1 (5.6%) was suggestive of hemangioma.
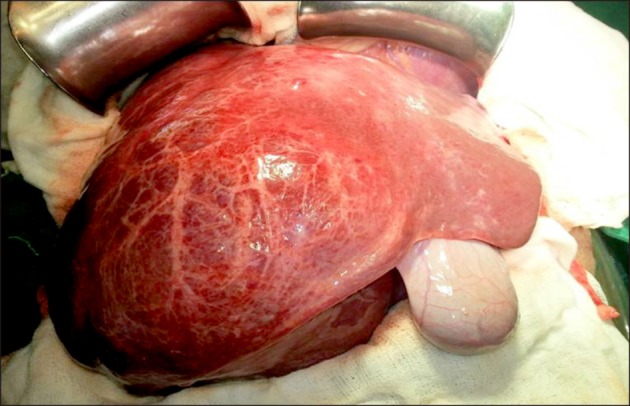
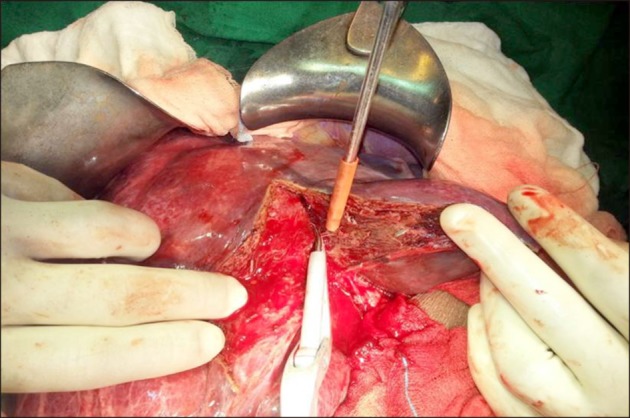
All patients underwent extra-capsular excision of the tumor (Figs. 1, 2). The median operating time was 180 minutes, (range 75 to 460 minutes). Median blood loss was 950 ml (range 100 to 3,500 ml). Six (33.3%) patients required intra-operative transfusion. Median post-operative stay was 5.5 days (range 3 to 10 days).
Fourteen (77.8%) had no post-operative complications. The major complications included one (5.6%) patient who required re-exploration for postoperative hemorrhage (CD grade IIIb) and one (5.6%) who had postoperative purulent intra-abdominal collection requiring per-cutaneous drainage (CD grade IIIa). There was no post-operative mortality. Postoperative day-3 liver function tests were within normal limits.
Histopathological evaluation of all 18 patients showed presence of cavernous hemangioma. Fifteen patients (83.3%) had a single lesion, whereas 3 (16.6%) had >1 lesions. Median size of hemangiomas was 9.9 cm (range 3.2 to 24 cm). Sizes of tumor and outcomes are shown in Table 2 and 3.
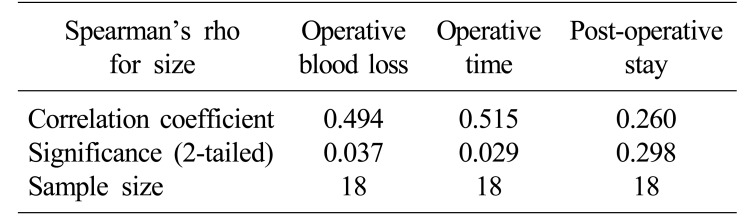
On correlating the size of the tumor with the duration of surgery, operative blood loss, and postoperative stay, the Spearman coefficient was found to be 0.515, 0.494, and 0.260 respectively; duration of surgery and operative blood loss showed significant correlation (p<0.05), indicating that the size of the hemangioma affected intraoperative parameters. The size of the tumor did no correlate significantly with postoperative complications (p=0.135; 95% CI=−1.66 to 11.29)
DISCUSSION
Hepatic hemangioma accounts for almost 75% of benign liver tumors, with a frequency of 0.4%to 7.3% at autopsy.9 These tumors are more commonly found in women, with a female: male ratio of up to 5:1.10 A female predisposition was seen in our experience (female: male ratio of 1.57:1), though not to the same extent.
Most authors label the hemangioma ‘giant’ if it is more than 10 cm.561112 However, it has been proved in multiple studies that size has no direct correlation with the extent of pain, and small lesions can also continue to have severe pain.3 A study by Etemadi et al.3 reported that 58% of the patients had abdominal pain at presentation, and in 50% of cases this pain was the reason for referral, which led to the diagnosis of liver hemangioma. However, in only 12.6% of the cases could the pain be attributed to the hemangioma. Pain most commonly results from the tumor stretching the liver capsule or compressing adjacent organs. Rarely has it been reported to be caused by infarction and necrosis of the tumor. In our series of 18 hemangiomas undergoing surgical resection, we found that 88.9% of patients were symptomatic with abdominal pain or mass per abdomen.
Uncommon complications of hemangioma include spontaneous rupture and malignant transformation, both of which are very rare.3 Until now, less than 50 cases of spontaneous rupture have been reported, and malignant transformation is practically nonexistent.
The ideal indication for surgery remains strictly related to symptoms and complications. The size of the tumor alone doesn't justify treatment. Yoon et al.7 evaluated 115 patients and found that the most common indication for surgery was the presence of symptoms (60%), with the other 40% being increasing size, large size, and uncertainty in diagnosis. In our study, 6 (33.3%) patients had atypical imaging characteristics, leading to diagnostic uncertainty; hence a surgical resection was considered for these patients.
Liver resection and enucleation are the two most common modalities of surgical management and have been the subject of multiple studies. Zimmermann and Baer4 described the well-formed tumor-liver interface and its surgical application. The space between the liver and the hemangioma is avascular, consisting of only liver tissue compressed by the growing hemangioma. No bile ducts and only a few blood vessels traverse the capsule, and these are easily controlled. By identifying this layer between the capsule of the hemangioma and the liver, one can remove the tumor with minimal risk of bleeding and postoperative bile leak. The amount of normal-functioning liver parenchyma removed is also minimal. This is, however, not possible for formal liver resections, because it entails transecting through the normal liver, with chances of increased blood loss and higher incidence of post-operative bile leaks. Singh et al.13 have found lesser blood loss with enucleation than with resections (400 ml vs. 1,300 ml) and shorter hospital stay (5 vs. 10 days). Resection remains the choice for multiple hemangiomas of the liver and for deep-seated hemangiomas where enucleation is not possible. In our study, all 18 patients underwent surgical excision of hemangioma by extra-capsular excision. It is safe and technically feasible in superficial as well as in large tumors with deep parenchymal extension. Excision of the hemangioma in the extra-capsular avascular plane minimizes the bleeding and bile leak. This procedure also allows excision of large hemangiomas without any parenchymal loss, post-operative liver functions are well preserved, and complications are minimized.
In our study, we also found that the larger is the tumor, the longer is the operative time and the greater is operative blood loss. Size of tumor, however, did not have any negative effect on perioperative complications.
The limitation of our study was the small sample size of eighteen patients analyzed retrospectively. However, hemangiomas are rarely treated by surgery; hence this analysis throws light on important parameters that guide decisions in management of these tumors, as well as on the technique of extra-capsular excision, which is a safe and effective approach that preserves maximal liver parenchyma with resultant early post-operative recovery.
In conclusion, surgical treatment of hemangiomas should be guided by the presence of symptoms or of diagnostic uncertainty, not by size alone. The size had no correlation with perioperative complications. The technique of extra-capsular excision is safe and technically feasible for most of the hemangiomas. This technique preserves maximal liver parenchyma, resulting in early post-operative recovery with minimal morbidity.

 XML Download
XML Download