

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is one of the common malignancies in women worldwide with more than 500,000 new cases diagnosed annually and approximate 250,000 related deaths each year [1]. The advent of well-developed cervical screening programs has reduced the incidence of cervical squamous cell carcinoma (SCC) substantially [2]. However, the incidence of cervical adenocarcinoma (AC) has increased in recent decades with the increase in oral contraceptive use, obesity, nulliparity and human papillomavirus infections. Cervical SCC accounts for approximately 75% of all cases of cervical cancer, whereas cervical AC accounting for approximately 20% to 25% [3456].
The epidemiology, clinicopathological and molecular characteristics, treatment response, and prognosis of cervical AC and SCC are different [78910]. In early-stage cervical cancer, randomized trials have demonstrated similar survival outcomes between surgery and definitive radiotherapy groups in SCC subtype, and surgery improved survival significantly compared to definitive radiotherapy in cervical AC [1112]. However, the treatment strategies are similar between cervical AC and SCC in the current National Comprehensive Cancer Network (NCCN) and Gynecologic Cancer Inter Group (GCIG) guidelines [1314].
Several retrospective studies have found that cervical AC patients treated with definitive or postoperative radiotherapy had a worse survival than cervical SCC patients [1516171819]. Our previous population-based study also found that surgical treatment was associated with better outcome in early-stage cervical AC compared with definitive radiotherapy [20]. Therefore, cervical AC may be resistant to radiotherapy [21], and surgical treatment may be the optimal treatment for early-stage cervical AC. However, many of the single-institution studies included small numbers of patients. In addition, studies focused on assessing patients with early-stage disease are limited. The purpose of our population-based study was to investigate the effect of histologic subtype on survival in node-negative, early-stage cervical cancer after hysterectomy.
MATERIALS AND METHODS
1. Patients
Patients with a primary diagnosis of cervical AC and SCC between 1988 and 2013 were included using the Surveillance, Epidemiology, and End Results (SEER) database [22]. We selected patients according to the following criteria: patients with International Federation of Gynecology and Obstetrics (FIGO) stages I–IIA cervical cancer; patients with cervical SCC and AC who received hysterectomy including lymphadenectomy; patients with pathologically node-negative disease; those who had not received preoperative or postoperative radiotherapy. The ethics committees of the First Affiliated Hospital of Xiamen University approved this study (approval number of institutional review board, 2015J01550).
2. Variables
The following demographic and clinicopathological variables were included: age, year of diagnosis, race/ethnicity, tumor grade, histologic subtype, FIGO stage, and survival. The primary endpoint of this study was cause-specific survival (CSS) and overall survival (OS). CSS was calculated for patients who were died of cancer related disease. OS was estimated from the date of treatment initiation to either the date of death or last follow-up.
3. Statistical analysis
All statistical analyses were performed using the SPSS statistical software package (version 21.0; IBM Corporation, Armonk, NY, USA). Comparisons between histologic subtypes in the demographic and clinicopathological variables were analyzed. Survival analysis was performed for all patients and for a subset of propensity score-matched patients. Propensity score matching (PSM) was performed using SPSS to create balanced cohorts of patients with cervical SCC and AC. The variables of age, year of diagnosis, race/ethnicity, tumor grade, FIGO stage, and number of removed lymph nodes (RLNs) were selected as pre-test covariates in PSM with an algorithm of 1:1 matching. The survival curves were calculated and compared using the Kaplan-Meier method and the log-rank test, respectively. Univariate and multivariate Cox regression analyses were used to explore the risk factors for CSS and OS. p<0.05 was considered significant for all analyses.
RESULTS
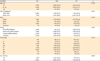
A total of 9,858 patients were identified: 6,117 patients (62.1%) and 3,741 patients (37.9%) with cervical SCC and AC, respectively. Table 1 lists the patient characteristics. Compared with cervical SCC, cervical AC cases were more likely to be younger (41–65 years), diagnosed after 2000, white, and have well-differentiated and FIGO stage IB1 disease. A total of 3,998 patients were fully matched in PSM: 1,999 (50.0%) and 1,999 (50.0%) patients with cervical SCC and AC, respectively. The groups were comparable in terms of age, year of diagnosis, race/ethnicity, tumor grade, FIGO stage, and number of RLNs (Supplementary Table 1).
Table 1
Patient characteristics
The median follow-up of the entire cohort was 97 months (range, 0–311 months). Survival analysis of the entire cohort determined that the 10-year CSS and OS rates were 93.9% and 90.5%, respectively. For SCC and AC, the 10-year CSS rates were 93.4% and 94.7%, respectively (log-rank test, p=0.011), and the 10-year OS rates were 89.6% and 92.2%, respectively (log-rank test, p<0.001). However, in the propensity score-matched cohort, there was no significant difference between AC and SCC in terms of CSS (log-rank test, p=0.336) (Fig. 1A) and OS (log-rank test, p=0.743) (Fig. 1B).
Fig. 1
Impact of histologic subtype on CSS (A) and OS (B) after PSM.
AC, adenocarcinoma; CSS, cause-specific survival; OS, overall survival; PSM, propensity score matching; SCC, squamous cell carcinoma.

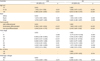
The univariate and multivariate prognostic analyses of patients with known demographic and clinicopathological variables were examined (n=7,534). Table 2 lists the univariate analysis results of the entire cohort. Age, ethnicity, tumor grade, FIGO stage, and histologic subtype were prognostic factors of CSS and OS; the number of RLNs was also a prognostic variable of OS. In the multivariate analysis, age, ethnicity, tumor grade, and FIGO stage remained independent prognostic factors of CSS and OS (Table 3), but histologic subtype was not associated with CSS (hazard ratio [HR]=1.146; 95% confidence interval [CI]=0.924–1.420; p=0.214) and OS (HR=0.989; 95% CI=0.833–1.175; p=0.904). In the propensity score-matched population, univariate and multivariate analyses showed that histologic subtype was not associated with CSS and OS (Supplementary Tables 2 and 3).
Table 2
Univariate analysis of prognostic factors

Table 3
Multivariate analysis of prognostic factors
DISCUSSION
In this study, we used the SEER database to analyze the prognostic role of histologic subtype including SCC and AC in patients with node-negative, early-stage cervical cancer after hysterectomy. We found that the AC subtype was not associated with worse survival compared with the SCC subtype. The propensity score-matched analysis also showed that survival was similar between the 2 groups.
The relative and absolute incidence of cervical AC has been increasing in recent decades [3456]. There is a potential difference in the clinicopathological characteristics of patients with cervical AC and SCC. Winer et al. [4] found that cervical AC tends to be well-differentiated, while cervical SCC features larger tumors and deeper invasion. In our study, cervical AC cases were more likely to be younger, diagnosed after 2000, white, and have well-differentiated disease, which is similar to our previous findings [19]. Due to the limitations of the SEER database, we could not obtain the lymphovascular invasion (LVI) status of the patients. However, previous studies have found no difference in LVI status between patients with early-stage cervical SCC and AC [423].
The treatment strategies in cervical AC are similar to cervical SCC in the current NCCN and GCIG guidelines [1314]. However, the local treatment strategies may lead to survival differences between cervical AC and SCC. A previous SEER study found that survival in cervical AC was worse compared with SCC in both early and advanced disease [24]. However, the study did not perform subgroup analysis of the effect of local treatment on survival. Several studies including ours have found that in patients who received definitive radiotherapy or adjuvant radiotherapy (high-risk factors), AC subtype was associated with worse survival compared with SCC subtype, whereas histologic subtype did not affect the survival outcome of patients with low-risk group after radical hysterectomy [192526272829]. Therefore, cervical AC may be resistant to radiotherapy, and surgical treatment may be the optimal treatment for early-stage cervical AC.
At present, only one randomized trial has shown that surgery has significantly better outcomes than primary radiotherapy in cervical AC, and long-term follow-up studies have yielded similar results [1112]. In our previous retrospective study, we also found that primary surgery produced significantly better outcomes than primary radiotherapy in early-stage cervical AC [20]. Therefore, survival may be similar in early-stage cervical SCC and AC after radical surgery. Several studies confirm our hypothesis, showing that there are no significant differences in survival between early-stage cervical SCC and AC after radical hysterectomy with lymphadenectomy [42327303132]. Our findings support the hypothesis that patients with cervical AC have distinct clinical outcomes from patients with cervical SCC following the different treatment strategies.
In this population-based study, we included patients with FIGO stages I–IIA cervical cancer who had undergone hysterectomy with lymphadenectomy, and we ruled out patients with node-positive disease and patients who had undergone preoperative or postoperative radiotherapy. Univariate analysis found that survival in cervical AC was better than that in cervical SCC, which may be attributed to the fact that the patients with cervical AC were younger, had later year of diagnosis, were white, and had well-differentiated disease. However, multivariate and PSM analyses did not reveal an adverse effect of histologic subtype on survival. These results suggest the influence of other high-risk clinicopathological factors rather than histologic subtype in early-stage cervical cancer after hysterectomy with lymphadenectomy.
Several limitations in our study should be acknowledged. First, there may have been potential confounding biases in this retrospective study. Second, although there was no significant difference in outcome between the 2 histologic subtypes, we were able to obtain the patterns of local and distant recurrence. Third, the SEER database does not contain information on pathological factors such as LVI, margin status, parametrial invasion, and cervical stromal invasion depth. Finally, the SEER database also lacks the details of adjuvant chemotherapy after hysterectomy, which may be a bias in our study.
In conclusion, our results suggest that cervical AC has equivalent survival to cervical SCC in patients with node-negative, early-stage cervical cancer after hysterectomy and lymphadenectomy. Our results may be useful for improving tailored treatment strategies and individualized follow-up planning for each cervical cancer histologic subtype.
 XML Download
XML Download