

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2009, the International Federation of Gynecology and Obstetrics (FIGO) revised FIGO staging of gynecologic malignancies including cervical cancer [1]. The descriptions for stage 0 and stage IIA were changed, whereas other stages including stage IIB–IVA remained the same. For stage III cervical cancer, invasion of tumor to only the lower third of vagina is considered stage IIIA. However, extension to only the lower third of vagina but not the pelvic sidewall is the least common in stage III with no more than 5% of patients in this stage [2345], and there are also limited studies of treatment outcomes in these patients. Some authors reported that stage IIIA had better treatment results than stage IIIB [67], whereas others showed the poorer overall survival (OS) of stage IIIA comparing with stage IIIB [28].
For stage IIIB, there are variations of the disease including tumor invasion to pelvic sidewall and/or with hydronephrosis status and with or without the lower third of vaginal invasion (LTI). In addition to extension of tumor to adjacent organs, prognosis of cervical cancer is also dependent on lymph node involvement [9]. In general, regional lymph nodes of cervical cancer are groups of pelvic lymph nodes and defined as stage IIIB in tumor, node, and metastasis (TNM) staging system. Whereas metastasis to other lymph nodes such as inguinal and para-aortic is determined as stage IVB and is not considered to be curative. In stage IIIB cervical cancer patients with LTI, there are chances of the disease spreading to superficial inguinal nodes. For this reason, the traditional field of external beam radiation therapy (EBRT) for stage IIIB with LTI is whole pelvis with lateral extension to inguinal area to prevent metastasis [10]. In addition, narrowing of vagina from invasion of tumor may cause improper intracavitary brachytherapy (ICBT) leading to insufficient amount of radiation. Therefore, these patients not only have chances to metastasize out of pelvis via superficial inguinal lymph node, but also have higher risk of persistent or local recurrence (LR) due to an insufficient treatment of brachytherapy.
At present, there is no study regarding stage IIIB patients with LTI, while few studies of stage IIIB cervical cancer patients with hydronephrosis status which is one of the variation of stage IIIB were reported [1112]. Therefore, the aim of this study was to ascertain whether treatment outcomes are different between stage IIIB cervical cancer patients with or without tumor extension to the lower third of vagina.
MATERIALS AND METHODS
1. Patients and methods
This study was the retrospective cohort study of stage IIIB cervical cancer patients who received radiotherapy at Faculty of Medicine Vajira Hospital between January 1995 and December 2012. All data were collected after an approval from the Ethics Committee for Research involving Human Subjects of the institution. Inclusion criteria were patients with confirmed pathological results of squamous cell carcinoma (SCC) or adenocarcinoma (ADC)/adenosquamous carcinoma and received a complete radiation therapy (RT) composed of EBRT and ICBT as planned. In accordance with FIGO staging system, all patients were obtained pelvic examination and bimanual rectal examination to determine extension of disease by both radiation oncologists and gynecologic oncologists. Computed tomography (CT) of abdomen and pelvis was not routinely performed and was not used for diagnosis of the local extension nor for staging. Patients with inguinal or para-aortic lymphadenopathy diagnosed by physical examination or CT were excluded. We matched one stage IIIB cervical cancer patient with LTI with 2 cervical cancer patients in the same stage without LTI. The first factor for matching was treatment modalities as RT alone vs. concurrent chemoradiation therapy (CCRT). Pathological results (SCC vs. ADC/adenosquamous carcinoma), age (no more than 5 years difference) and year that patients received the treatment (no more than 5 years apart) were attempted to match afterwards. Treatment outcomes of patients were blinded during matching process to prevent selection bias. Other data collected were hemoglobin (Hb) level (before treatment), total treatment time (TTT) from the first day of starting treatment to the last day of ICBT, results of the treatment including response to radiotherapy (persistent or complete response), rate of LR, rate of distant metastasis (DM), progression-free survival (PFS), OS as well as side effects from radiotherapy at bladder and large bowel.
2. RT and chemotherapy
The standard treatment of RT for stage IIIB cervical cancer patients with or without LTI is same in our institution. Two-dimensional EBRT with a total dose of 40–46 Gy (2 Gy/fraction) was applied to the whole pelvis and then boosted up to parametria and pelvic sidewalls to 54–60 Gy. Four to 6 fractions of high dose rate (HDR) ICBT with weekly fractions of 6.5–7.0 Gy to point A (pear-shaped isodose distribution) were applied at about the 4th-week of EBRT. The difference of treatment between those 2 groups was the field of EBRT in terms of lower border of whole pelvis, which had to cover along vagina for patients with LTI. The prophylaxis inguinal irradiation was not adopted for all patients. Distribution of HDR ICBT was dependent on the remaining vaginal lesion at each time of ICBT. If lesion remained, a vaginal cylinder was applied together with conventional tandem and ovoid or later as appropriate. Source of brachytherapy was extended from cervical os to the lower border of lesion (galaxy-shaped isodose distribution). In patients who received CCRT, platinum-based regimens were used. During 17-year period of this retrospective study, variable regimens of chemotherapy were used for CCRT. However, all 102 patients received platinum-based regimen including weekly carboplatin (64/102), weekly cisplatin (22/102), combination of carboplatin and 5-fluorouracil (5-FU) every 28 days (7/102), combination of cisplatin and 5-FU every 28 days (5/102), and cisplatin every 3 weeks (4/102).
3. Assessment of treatment outcomes
After completion of treatment, all patients were followed up to receive pelvic examination at the first 1–2 months and then every 3–6 months until death. Persistent disease was determined from pelvic examination and confirmed by biopsy at 3 months after completion of treatment. LR was the emergence of the disease at cervix, vagina or pelvis. DM was determined as presence of disease outside the pelvis. CT and other imaging were performed in patients suspected to have LR or DM.
4. Statistical analysis
SPSS statistical software version 11.5 (IBM Corp., Chicago, IL, USA) was used for data analysis. Quantitative data were presented by mean or median as appropriate, and qualitative data were presented as percentage. OS and PFS were analyzed by the Kaplan-Meier method and compared between both groups by log rank test. The Cox proportional hazards model was used to adjust all prognostic factors. A 2-sided p-value <0.05 was considered statistically significant.
RESULTS
During the study period, 380 stage IIIB cervical cancer patients were identified and 72 patients had LTI (18.9% of stage IIIB). After matching between one stage IIIB cervical cancer patient with LTI with 2 patients in the same stage without LTI, 216 patients were included in this study (72 with LTI and 144 without LTI) with the mean age of 55.9±11.1 years. One hundred and fourteen patients (52.8%) received only RT and 102 patients (47.2%) received CCRT. Pathological results confirmed that 83.8% of these patients had SCC and 16.2% had ADC. Each matching factor including treatment modalities, histopathology, age, and treatment year was comparable. Baseline characteristics of patients and treatment are listed in Table 1. Mean of TTT was 56.7±10.9 and 59.0±13.0 days in stage IIIB patients without LTI compared with those who had LTI, respectively.
Table 1
Baseline characteristics of stage IIIB cervical cancer patients

After completion of treatment, the percentage of patients with persistent disease was significantly higher in patients with LTI than patients without LTI with 19.4% (14/72) and 6.3% (9/144), respectively (odds ratio [OR]=3.62; 95% confidence interval [CI]=1.48–8.84) (p=0.005). For treatment modalities, the percentage of persistent disease in patients who received RT alone at 11.4% (13/114) and those who received CCRT at 9.8% (10/102) was not significantly different (p=0.826). Although patients whose histopathology was ADC were likely to have higher persistent disease than those with SCC, 17.1% (6/35) vs. 9.4% (17/181), there was no statistical significance (p=0.174).
Median follow-up in this study was 9.7 years (range, 2.0–19.9 years). After treatment, 45 patients died from unknown causes, and 5 patients were untraceable. Out of 45 patients who died from unknown causes, 29 died within 5 years after the treatment (cause of death was likely to be cervical cancer; censored as death from disease) and 16 died at more than 5 years after the treatment (cause of death was likely to be other diseases; censored as no disease). Therefore, there was no data about areas of treatment failure for 34 patients (29 died within 5 years and 5 had no data). Causes of treatment failure from 182 patients (121 patients without LTI and 61 patients with LTI) who had recorded document were 8.8% (16/182) with local progression from persistent disease, 3.8% (7/182) with persistent of the disease with later development of DM, 8.2% (15/182) with only pelvic recurrence, 22.5% (41/182) with only DM, and 2.7% (5/182) with both pelvic recurrence and DM. When we compared these treatment outcomes between patients without and with LTI, local failures from treatment (persistent disease and pelvic recurrence) were 18.2% (22/121) and 34.4% (21/61), respectively (OR=2.36; 95% CI=1.17–4.77) (p=0.017). Sixty-one patients with LTI were divided by type of applicators into 2 large groups including vaginal cylinder vs. tandem and vaginal cylinder/tandem and ovoid/tandem, ovoid, and vaginal cylinder. The treatment outcomes of these 2 groups were compared. LR was found in 3 out of 4 patients (75.0%) with application of vaginal cylinder, and 18 out of 57 patients (31.6%) were applied with other applicators (OR=6.50; 95% CI=0.63–66.89). However, there was no statistical significance (p=0.113). While rate of DM of patients without LTI was rather equal to patients with LTI, 28.9% (35/121) vs. 29.5% (18/61), respectively (p=1.000). The most common site of DM was para-aortic lymph node accounted for 16.5%. Other sites of distant failure were lung (9.9%), liver (7.7%), supraclavicular lymph node (7.1%), bone (4.9%), brain (1.6%), and inguinal lymph node (1.1%). Distant recurrence at inguinal lymph node occurred in only 2 patients without LTI.
At the end of the study, 59 patients (27.3%) were still alive without documentation of disease recurrence, and 82 patients (38.0%) died from cervical cancer (Table 2). The median OS of patients without LTI was 52.8 months compared with 22.1 months in those with LTI. The 2- and 5-year OS of patients without LTI were 66.5% and 46.8%, respectively compared to those with the invasion accounted for 50.0% and 28.9%, respectively (p=0.003). The similar result can be observed when compared the 2- and 5-year PFS of patients without LTI to those with the invasion. The percentages of 2- and 5-year PFS of patients without LTI were 61.6 and 46.6, respectively. On the other hand, patients with the invasion had 44.4% and 28.9% of 2- and 5-year PFS, respectively (p=0.002). Univariate and multivariate analysis of the data suggested that LTI was the only factor affected survival outcomes (Tables 3 and 4). Late grade 3–4 side effects of large bowel and bladder were 9.7% and 3.7%, respectively. Six patients without LTI (4.2%) and 5 patients with the invasion (6.9%) died from those late complications (Table 2).
Table 2
Status of patients
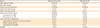
Table 3
Factors affected treatment outcomes: univariable analysis
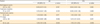
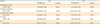
Table 4
Factors affected treatment outcomes: multivariate analysis
DISCUSSION
Stage III cervical cancer patients, which are classified by FIGO according to their clinical appearances, are divided into stage IIIA and IIIB. Patients with stage IIIB accounted for higher ratio than stage IIIA have different severity of invasion including pelvic sidewall invasion, pelvic sidewall invasion with LTI, pelvic sidewall invasion with presence of hydronephrosis, or combination of pelvic sidewall invasion with presence of hydronephrosis and LTI; these factors have effects on the variation of survival outcomes. Regarding the impact of hydronephrosis status, univariate analysis from the study of Rose et al. [11] showed that this factor affected OS and PFS. On the other hand, there was no statistical significance of these results when multivariable analysis was used, suggesting that this factor is not prognostic.
This is the first study that compared stage IIIB cervical cancer patients with invasion to pelvic sidewall only with those who had invasion to pelvic sidewall and the lower third of vagina. The rate of patients with LTI was 18.9% in stage IIIB cervical cancer patients. We found that invasion to the lower third of vagina is a substantial prognostic factor for both OS and PFS when the data was analyzed by univariate and multivariate analysis. Stage IIIB cervical cancer patients with LTI had 1.63 times higher death rate than those who had invasion to pelvic sidewall alone. Other factors such as treatment modalities (RT alone vs. CCRT) and pathological results (SCC vs. ADC) had no impact on treatment outcomes, which was consistent with our previous study [13]. That the proportion of patients who had Hb levels less than 10 g/dL before treatment was higher in those with LTI suggests the difference in aggressiveness of disease. However, there was no statistical difference in proportion of patients with low Hb level in multivariate analysis. This result was different from the previous studies which included patients with other stages and Hb levels were not analyzed separately according to the stage [131415].
The influence of TTT over 56 days was observed in univariate analysis for PFS. We found that patients with LTI who experienced several fractions of brachytherapy had higher chance to have TTT over 56 days than patients without LTI. However, this effect could not be demonstrated when all factors were adjusted. The long treatment period from more fractions of brachytherapy in patients with LTI may be overcome by the accelerated repopulation of cancer cells. TTT over 56 days had no effect on survival outcome in this study.
The persistence of the disease after completion of treatment in patients with LTI was 3.62 times higher than that of patients with invasion to pelvic sidewall only. Notably, these patients had 2.36 times more chances to develop local progression and produced cause of death later. The main cause of local failure was likely due to inadequate treatment for local disease. The local failure rate of patients with application of vaginal cylinder was 6.5 times higher than patients who received other applicators. Due to the small number of patients in this group, there was no statistical significance. On the other hand, invasion to the lower third of vagina had no effect on DM. Metastasis of the disease in these 2 groups of patients had a similar ratio at around 30%. Therefore, these data suggested that control of the disease at pelvis in these patients had an effect on long-term survival rate of the patients.
The limitation of this study is that CT-scan after completion of treatment was not routinely used to follow-up for all patients. Rate of local and distant failure presented in this study might be underestimated. Moreover, there were 29 patients who died with unidentified causes within 5 years as well as 5 patients whose data were untraceable. Thus in this study, these patients were regarded to have succumbed to cervical cancer. However, 5-year OS in patients without LTI in our study which was approximately 50%, was similar to that of the patients without hydronephrosis reported by Rose et al. [11].
There are few studies in stage IIIA cervical cancer patients which demonstrated the conflict of results when compared with stage IIIB. Five-year OS of stage IIIA patients in this study was higher than that of stage IIIB with 58%–62% and 34%–50% [67], respectively. Other studies, on the other hand, reported that 5-year OS of stage IIIA was less than stage IIIB. Hiilesmaa et al. [2] reported that 5-year OS of stage IIIA and stage IIIB were 9% and 33%, respectively. Similar result was also reported by Montana et al. [8], which showed that 5-year OS of stage IIIA was 26%, and stage IIIB was 35%. On a report of 1992, there were 44 patients (3%) with stage IIIA out of 1,473 stage III cervical cancer patients [5]. All patients received RT and 9 patients (approximately 20%) received EBRT only due to spreading of the disease causing vaginal narrowing and failure of ICBT. The 5-year OS in these patients was 37%. As a result, a pivotal point of cervical cancer stage IIIA or IIIB is LTI due to an insufficient radiation dose from EBRT and ICBT to cover the extended lesion. Unfortunately, those patients with persistence of the disease at vagina were not likely to receive salvage surgery and would end up with progression of the disease. In 2015, Rose et al. [16] generated nomograms for predicting 2-year PFS, 5-year OS and pelvic recurrence in stage IB–IVA cervical cancer. They reviewed 2,042 locally advanced cervical cancer patients who were included in 6 studies of Gynecologic Oncology Group. From data analysis, there were common 6 significant prognostic factors, which were composed of all 3 models including histology, performance status, tumor size, FIGO stage, pelvic node, and treatment. Summation of points for each factor reflected the foresight of treatment outcomes, and high points indicated worse outcomes. The number of patients in stages IIIA and IIIB in that study was 1.1% and 27.7%, respectively. Importantly, stage IIIA had higher points than stage IIIB for all nomograms, and was the worst factor for predicting 5-year OS and pelvic recurrence [16]. This finding emphasized the significance of LTI to survival outcomes, which was the main diagnostic feature for stage IIIA as well as one of the conditions for stage IIIB.
At present, this study was the first study demonstrated different treatment outcomes of stage IIIB cervical cancer patients with LTI and patients in the same stage without LTI. Although FIGO revised staging system for cervical cancer in 2009, classification of stage III cervical cancer remains the same which cannot represent the real prognosis for all patients in stage III. The finding from our study may be useful to reflect the necessity of stage revision for stage III cervical cancer; stage IIIA should be cervical cancer with only invasion to pelvic sidewall or with presence of hydronephrosis, and stage IIIB should be cervical cancer with LTI with or without invasion to pelvic sidewall or with presence of hydronephrosis. It is probable that this new classification is more precise to predict the pattern of treatment failure and survival outcomes for stage III cervical cancer patients than FIGO 2009. Although nowadays, the modern techniques of EBRT such as intensity-modulated radiation therapy (IMRT) are developed for many types of cancer, IMRT is not the standard technique for locally advanced cervical cancer [17]. Moreover, the proper position of applicator and packing for ICBT has limitation from narrowing of vagina due to the disease, and dose prescription at point A may be compromised. These patients may need interstitial brachytherapy to enhance local control. Insufficient radiation dose for tumor with high chance of toxicity for normal organs frequently occurrs in cervical cancer patients with LTI. For modern technique of brachytherapy, few studies reported impressive results including good local control rates and low toxicities when using image-guided brachytherapy (IGBT) in locally advanced stage of cervical cancer [181920]. However, it is not proved by randomized phase III study comparing between the conventional ICBT (2-dimensional brachytherapy) with IGBT about their efficacy and effectiveness. Therefore, more studies especially IMRT for boost to vagina, interstitial brachytherapy and IGBT are still needed to explore the appropriate treatment for patients with LTI to improve their local control, which later can enhance the survival outcomes in the long-term.
To conclude, invasion of tumor to the lower third of vagina is a poor prognostic factor for stage IIIB cervical cancer patients. The main treatment failure is persistence of disease and pelvic recurrence. It might be appropriate to subdivide FIGO stage IIIB cervical cancer to IIIB1 involving up to pelvic sidewall or hydronephrosis and stage IIIB2 involving up to pelvic sidewall or hydronephrosis with LTI.
 XML Download
XML Download