

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Establishment of obligate cause of carcinogenic human papillomavirus (HPV) to cervical cancer contributed to an increasing shift from cytology-based cervical cancer screening to HPV-based molecular technique worldwide [123]. A growing body of evidence showed superior sensitivity of HPV testing to cytology for detection of moderate or severe cervical intraepithelial neoplasia (CIN) [456]. Well-organized single round HPV testing could substantially decrease cervical cancer mortality in low-income countries [78].
Currently, much evidence on the clinical value of HPV-based cervical cancer screening is based on studies using hybrid capture 2 (HC2) test (HC2 test; QIAGEN Inc., Hilden, Germany; formerly Digene Corporation), which was the first commercial HPV testing approved by Food and Drug Administration (FDA) and collectively targeted 13 carcinogenic HPV types without discerning individual genotype [910]. SPF10-line probe assay (LiPA) system (DDL Diagnostic Laboratory, Rijswijk, the Netherlands), based on broad spectrum amplification of DNA with SPF10 as primers and reverse linear probe hybridization, has been widely used in clinical trial of HPV vaccination for research of identification of specific sequences in the L1 region of the HPV genome of 28 HPV types [11]. Previous studies have reported good agreements between HC2 and SPF10-LiPA system in detecting carcinogenic HPV genotypes among young women aged 18–25 or under a colposcopy referral setting [1213]. However, few studies have prospectively evaluated the effect of discordant results of HC2 and HPV genotyping by use of SPF10-LiPA on the detection of cervical cancer and precancer, i.e., HC2 positive but non-carcinogenic HPV positive identified by SPF10-LiPA, indicating cross-reactivity in HC2 testing, which would provide more detailed information for clinical performance of HC2 assay in cervical cancer screening.
In the present study, based on a ten-year follow-up cohort among Chinese women, we sought to analyze discordant HPV results between HC2 and SPF10-LiPA testing and particularly focused on the accumulative risk of cervical cancer for those infected with the cross-reacted HPV types of HC2 assay.
MATERIALS AND METHODS
1. Study population
In 1999, 1,997 non-pregnant women with no history of hysterectomy were enrolled in Shanxi Province Cervical Cancer Screening Study-I (SPOCCS-I) in Shanxi, China. Baseline details have been published previously [1415]. Three follow-ups to women with intact cervix were conducted in 2005, 2010, and 2014, respectively, in which HC2 assay, liquid-based cytology (LBC — ThinPrep®, Hologic, Bedford, MA, USA or SurePath™, BD Diagnostics, Franklin Lakes, NJ, USA) and visual inspection with acetic acid (VIA) were performed, except for VIA in 2014. Women with any positive screening result were referred to colposcopy. Biopsy was taken if necessary. Cytological results were interpreted by cytopathologists who were blinded to any other test results using the Bethesda classification system. Histological diagnoses were interpreted by histopathologists according to the CIN nomenclature. Histological diagnoses of CIN grade 2 (CIN2), CIN grade 3 (CIN3) or cervical cancer were categorized as CIN grade 2 or worse (CIN2+). This study was approved by Institutional Ethical and Research Reviews Boards of Cancer Institute/Hospital, Chinese Academy of Medical Sciences.
Data for the present study were obtained from two visits of SPOCCS-I study in 2005 and 2014 because no ThinPrep cytological specimens remained or were available for HPV genotyping in 1999 and 2010. A total of all 304 HC2-positive women in 2005, all 294 HC2-positive women in 2014 and 300 HC2-negative women randomly selected from two visits were included in final analysis.
2. HC2 assay for HPV DNA detection
We tested all cervical cytological specimens using HC2 according to the manufacturer's instructions. HC2 is based on hybridization of HPV DNA to a high-risk RNA probe cocktail that collectively targeted 13 high-risk HPV types (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) but does not discriminate individual genotypes. Using chemiluminescent measurements, this assay provides a semi-quantitative result with relative light units/cut-off (RLU/CO), which indicates HPV DNA viral loads in specimens. Measurements above the RLU/CO, equivalent to 1.0 pg/mL of HPV DNA (signifying at least 5,000 viral copies) were scored as HC2 positive. Positive and negative controls provided by the manufacturer were included in each run of test.
3. SPF10-LiPA for HPV genotyping
Well-preserved cytological specimens were tested by SPF10-LiPA system for HPV genotyping. Following the total DNA extraction from cells with Total Nucleic Acid Isolation kit (QIAGEN Inc.), SPF10 (DDL Diagnostic Laboratory) was used as polymerase chain reaction (PCR) primer set to amplify a small fragment of 65 bp from the L1 region of a broad spectrum of at least 54 HPV types. Because of its shorter amplification product, it is thought to be with higher analytic sensitivity but possibly lower specificity for HPV detection than DNA-based assays [16]. A reverse line probe assay (INNO-LiPA HPV Genotyping Extra; Innogenetics, Ghent, Belgium) is then performed to achieve genotype identification with a blank negative control. HeLa cell DNA (DDL Diagnostic Laboratory) was used as the positive control. Finally, hybridization results were visualized in purple color on the probe line and interpreted through comparison with reference cards. SPF10-LiPA Extra system version 2 (Innogenetics) used in this study was intended to detect 28 HPV types, including 13 carcinogenic types targeted by HC2 and 15 non-carcinogenic HPV types (HPV6, 11, 26, 40, 43, 44, 53, 54, 66, 69, 70, 71, 73, 74, and 82).
4. Statistical analysis
SPF10-LiPA results were classified into three levels: 1) LiPA-carcinogenic HPV positive: positive for any of the 13 types targeted by HC2; 2) LiPA-non-carcinogenic HPV positive: positive for 15 types not targeted by HC2; and 3) LiPA-HPV negative: HPV not detected by SPF10-LiPA. To compare HPV results by HC2 and SPF10-LiPA, 6 combinations of HC2 and SPF10-LiPA results were classified as follows: 1) HC2 positive and LiPA-carcinogenic HPV positive; 2) HC2 positive and LiPA-non-carcinogenic HPV positive; 3) HC2 positive but LiPA-HPV negative; 4) HC2 negative but LiPA-carcinogenic HPV positive; 5) HC2 negative but LiPA-non-carcinogenic HPV positive; and 6) HC2 negative and LiPA-HPV negative. Besides, LiPA-non-carcinogenic HPV positive and LiPA-HPV negative were grouped as LiPA-carcinogenic negative when estimating agreement on carcinogenic HPV results between HC2 testing and LiPA.
Agreement on carcinogenic HPV types between the two assays was determined with crude agreement and unweighted kappa statistics. McNemar's χ2 analysis was used to test the discrepancy between HC2 positive but LiPA-carcinogenic negative samples and HC2 negative and LiPA-carcinogenic negative samples. Meanwhile, considering the potential age effect on HPV results [13], we also conducted agreement analysis in three age subgroups (40–50, 51–60, and ≥61 years). Proportions of abnormal cytology results (atypical squamous cells of undetermined significance or worse, [ASCUS+]) and CIN2+ among 6 combinations groups were calculated to investigate cross-sectional association between HPV results of two assays and disease outcomes. HPV viral loads were logarithmically transformed to conform to normal distribution and compared among various combination groups using one-way analysis of variance (ANOVA) analysis and further comparison with Dunnett's test. Ten-year CIR of CIN2+ and corresponding 95% confidence interval (CI) in each combination group was estimated using Kaplan-Meier methods. Hazard ratios (HRs) of CIN2+ were estimated using Cox proportional hazard models with HC2 positive but LiPA-HPV negative samples as the reference. Positive percentage for each HPV type tested by HC2 was calculated to evaluate the possibility to cross-react with non-carcinogenic HPV types. All statistical tests were 2-side with 0.05 as the significant level and performed using SPSS 18.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. HPV detection by HC2 and SPF10-LiPA
We compared the HPV results of HC2 to those of SPF10-LiPA assay in the whole and also in three age groups (Table 1). The overall crude agreement between the two assays for carcinogenic HPV types was 73.27% (95% CI=70.29%–76.06%) and kappa value was 0.439, indicating acceptable agreement between 2 tests. Eighty women (8.9%) were HC2 positive but LiPA-non-carcinogenic HPV positive, caused by cross-reacted HPV types by HC2 assay. Similarly, 77 women (8.6%) were HC2 negative but LiPA-carcinogenic HPV type positive, suggesting the probably miss-to-detection types by HC2 assay. Crude agreement rate of carcinogenic HPV types in 2 older subgroups (51 years or older) were better than that in 45–50 years subgroup but no statistical significance was observed (78.07% and 75.41% vs. 70.14%).
Table 1
Carcinogenic HPV detection by HC2 and SPF10-LiPA in 898 specimens by age groups

Data shown are number (%) not otherwise specified.
CI, confidence interval; HC2, hybrid capture 2; HPV, human papillomavirus; LiPA, line probe assay.
*Negative by 13 HC2-targeted HPV types (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68); †No HPV detected by LiPA; ‡Positive by HPV6, 11, 16, 18, 26, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 66, 68/73, 70, 74, and 82; §Agreement and Kappa were estimated between HC2 testing results and LiPA-carcinogenic HPV results.
2. Cross-sectional cytology and histology outcomes in various combinations of HC2 and SPF10-LiPA results
ASCUS+ proportions differed by HC2 and SPF10-LiPA status (F=182.708; p<0.001), as presented in Fig. 1. Among HC2 positive women, the proportions of ASCUS+ in LiPA-carcinogenic HPV positive (56.4%) or LiPA-non-carcinogenic HPV positive women (50.0%) were statistically higher than that in LiPA-HPV negative women (13.6%) (both p values were less than 0.001). Furthermore, HC2 positive and LiPA-carcinogenic positive women presented higher high-grade squamous intraepithelial lesion (HSIL) proportions than other subgroups (all p values were less than 0.010, Supplementary Table 1). All HC2 negative women had relatively low ASCUS+ proportion ranging from 9.1% to 14.3%. However, no differences were found in HC2 negative women at other cytology cut-offs (Supplementary Table 1).
Fig. 1
Abnormal cytology and CIN2+ proportions stratified by various combinations of HC2 and SPF10-LiPA testing results.
ASCUS+, atypical squamous cells of undetermined significance or worse; <CIN2, not severe than cervical intraepithelial neoplasia grade 2; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HC2, hybrid capture 2; HPV, human papillomavirus; LiPA, line probe assay; NILM, negative for intraepithelial lesion or malignancy.
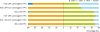
Histological CIN2+ proportions in various combinations of HC2 and SPF10-LiPA were also presented in Fig. 1. Almost all CIN2+ cases (96.4%) were detected in women concurrently positive by HC2 and LiPA-carcinogenic HPV. One CIN2 case was observed in HC2 positive but LiPA-HPV negative woman and one in HC2 negative and LiPA-HPV negative women. By contrast, HC2 positive and LiPA-non-carcinogenic women had high abnormal cytology proportion but developed less CIN2+ cases. No CIN2+ was found in HC2 negative but LiPA-carcinogenic women or HC2 negative but LiPA-non-carcinogenic women.
3. Viral loads in various combinations of HC2 and SPF10-LiPA results
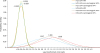
Log-transformed HPV viral loads in various combinations of HC2 and SPF10-LiPA test results were presented in Fig. 2 (with full detail in Supplementary Table 2). Among HC2 positive women, LiPA-carcinogenic HPV positive women had the highest viral loads while LiPA-HPV negative women had the lowest. HC2 positive and LiPA-non-carcinogenic positive women had the intermediate viral loads. However, no similar patterns were observed for HC2 negative women.
4. CIR of CIN2+ in various combinations of HC2 and SPF10-LiPA
Ten-year CIR of CIN2+ combining baseline study and follow-up and the corresponding HR stratified by HC2 and SPF10-LiPA status was presented in Table 2. Generally, HC2 negative test predicted extremely lower CIR of CIN2+ within 10 years than HC2 positive results (0.8% vs. 20.1%; χ2=27.149; p<0.001), irrespective of SPF10-LiPA status. Among HC2 positive women, CIR of CIN2+ remarkably differed by SPF10-LiPA test results (χ2=14.275; p=0.001). Women concurrently positive by HC2 and LiPA carcinogenic HPV conferred the highest CIR of CIN2+ 25.70% (95% CI=23.55%–27.91%) within 10 years and that for HC2 positive but LiPA-HPV negative women was 1.85% (95% CI=1.78%–1.92%). Of note, those HC2 positive and LiPA-non-carcinogenic HPV positive women also presented a notable high CIR of CIN2+ (9.97%; 95% CI=8.57%–11.50%). Conversely, no CIN2+ cases were detected within 10 years in HC2 negative and LiPA-HPV negative women or HC2 negative and LiPA-non-carcinogenic HPV positive women. Although one CIN2 case developed over 10-year follow-up in the HC2 negative but LiPA-carcinogenic HPV positive subgroups, the overall risk was very low with CIR of CIN2+ of 2.56% (95% CI=2.44%–2.70%).
Table 2
Ten-year cumulative risk of developing CIN2+ in various combinations of HC2 and SPF10-LiPA test results

We further analyzed the variation of HPV genotypes for those CIN2+ women with discordant HC2 and SPF10-LiPA results. Among 44 women in HC2 negative but LiPA-carcinogenic HPV positive subgroups, one CIN2 woman was initially co-infected with HPV58 and HPV44 with normal histology and then HPV58 at the time of CIN2 diagnosis after 5 years. Among 33 women in HC2 positive but LiPA-non-carcinogenic HPV positive subgroups, two women developed CIN2+ over ten years of follow-up. One was initially infected with HPV11 and then HPV16 at the time of CIN2 diagnosis after 5 years. The other was infected with HPV69 and HPV71 initially, and then HPV59 and HPV40 at the time of CIN3 diagnosis after 10 years.
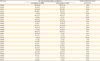
5. Cross-reactivity to untargeted HPV types by HC2
HC2 assay was originally designed for identification of 13 carcinogenic HPV types, but untargeted HPV types were also frequently detected by HC2, due to cross-reactivity of pooled probes. Table 3 presents the detecting ability to individual HPV type of HC2. Identification to different HPV types targeted by HC2 ranged from 74.5% (HPV56) to 100% (HPV35 and HPV45). Eighty-nine percent of the samples identified as HPV16 positive by SPF10-LiPA were tested positive by HC2 and 86% for HPV18. Overall, HC2 identification to untargeted HPV types ranged from 30.4% (HPV6) to 100.0% (HPV26, HPV73, and HPV82). HPV66, a probably carcinogenic type not targeted by HC2 probe, had a high possibility to be identified by HC2 (58.6%). Other common non-carcinogenic HPV types but detected by HC2 included HPV69 (84.0%), HPV71 (82.6%), HPV53 (78.9%), HPV11 (60%), HPV43 (60%), and HPV54 (60%).
Table 3
The positive likelihood of LiPA-carcinogenic and LiPA-non-carcinogenic HPV types tested by HC2 assay
DISCUSSION
In this study, based on a subpopulation from a prospective cervical cancer screening cohort with well-organized follow-up in China, we confirmed a reasonable agreement on detection of carcinogenic HPV between HC2 and SPF10-LiPA testing and revealed the accumulative risks to develop cervical cancer and precancers for women with different testing results between two assays. We took a particular interest in subsequent risks of CIN2+ for women with discrepant assay results. Our data showed that non-carcinogenic HPV types determined by SPF10-LiPA and cross-reacted by HC2, accounted for 8.9% specimens. These cross-reacted HC2 positive women would be confronted with great long-term risks of CIN2+ that should not be ignored, indicating potential benefit from the cross-reactivity. Meanwhile those negative by HC2 albeit carcinogenic HPV positive by LiPA remained low risk of CIN2+, providing great assurance against cervical cancer and precancers by negative HC2 results in cervical cancer screening.
HPV results tested by HC2 assay and SPF10-LiPA system have been previously compared but the agreement rates on carcinogenic HPV were slightly discrepant among studies [1213]. Safaeian and colleagues [13], using the data of women who participated in a randomized, double-blind, placebo-controlled phase III HPV16/18 Vaccine Trial at baseline in Guanacaste, Costa Rica, found a crude agreement of 88% between two assays whereas Chris Perrons, based on women referred to the colposcopy clinic, found an agreement of 70%. By contrast, our study, with the subpopulation composed of all HC2 positive specimens and some randomly selected HC2 negative specimens (the ratio was approximately 2:1) from 2 follow-up visits, revealed an agreement of 73% for carcinogenic HPV, which was extremely close to the findings of Chris Perrons' study [12]. Discrepancies on agreement among studies are probably due to variation of population with different HPV infection rate, sample size, and testing settings [1213].
Age and viral loads, previously reported to be associated with discordance of HC2 and SPF10-LiPA assays among young women [13], were further analyzed in our study among middle-aged women. Although Safaeian and colleagues [13] found that carcinogenic HPV positive identified by SPF10-LiPA but HC2 negative women were older than carcinogenic HPV negative identified by SPF10-LiPA but HC2-positive women, our study did not show such remarkable differences. Instead, we found similar detection rate of carcinogenic HPV at all age levels. Thus, we excluded the potential impact of host characteristics such as age on the analytic performance and confirmed the stability of HPV DNA test. HPV viral load, indicated by signal strength in HC2 test, reflects the productivity of DNA replication in HPV life cycle and defines the course of HPV infection [17]. In our study, HPV viral loads dramatically differed by SPF10-LiPA results in HC2 positive specimens while no similar patterns in HC2 negative specimens. We found that most HC2 positive but LiPA-carcinogenic HPV negative women were infected with low viral loads of HPV, which was consistent with Safaeian and colleagues' findings [13]. Considering that SPF10-LiPA specifically targets the L1 region of HPV genome while HC2 targets the whole length, further investigation into the change of molecular integration status of HPV DNA for specimens with low viral loads might be needed for the interpretation of these findings.
Different sensitivity to detect HC2 targeted genotypes and cross-reactivity with non-carcinogenic HPV types has been reported but reaching no unanimous conclusions [181920]. Our study found that among women positive by LiPA-carcinogenic genotypes, HPV35 and 58 were most likely to test positive by HC2 and among women positive by LiPA-non-carcinogenic genotypes, HPV82 and 73 were most likely to test positive by HC2, which coincided with the findings by Castle et al. [1920] using the PGMY09/11 L1 primer-based genotyping assays to detect the genotypes and with those by Preisler et al. [18] using CLART HPV assay to detect the genotypes. All HPV45 positive women were identified by HC2 in our study, however, only 72.7% were HC2 positive in Castle's study [19]. A possibility of 84.2% for HPV56, the second mostly likely HPV types detected by HC2, were identified in Castle's study [19], which was 74.5% in our study. Besides, other common non-carcinogenic types cross-reacted by HC2 were found to be HPV26, 69, 71, and 40 in our study but HPV11, 61, 67, 70, and 81 in Castle's study [20]. As a probable carcinogenic but not HC2-targeted HPV [21], HPV66, frequently reported to be cross-reacted by HC2 [202223], had the likelihood of 58.3% to be tested positive by HC2 in our study. The probability to cross-react with non-carcinogenic HPV genotypes greatly depends on analytic sensitivity of the intended tests used for HPV genotyping, which partially interpreted the discrepant findings among studies [181920]. Meanwhile cross-reactivity of HC2 with any non-carcinogenic type also disclosed a predilection of HC2 probe set to cross react with the HPV phylogenetic related clades that led to lack of perfect fidelity of the HC2 probe set [24].
The clinical implication of cross-reactivity by HC2 has been previously evaluated by calculating the sensitivity and specificity for the detection of high-grade cervical neoplasia from a cross-sectional perspective and little effect of cross reactivity with non-carcinogenic HPV types was found on the overall clinical performance of HC2 as a general screening test [20]. Few studies, however, gauged the potential clinical significance of this cross-reactivity of HC2 with non-carcinogenic HPV types for the prospective risk prediction of HPV testing for general screening. In our study those HC2 positive and LiPA-non-carcinogenic HPV positive women presented a noticeable subsequent CIN2+ risk within 10 years (9.97%; 95% CI=8.57%–11.50%), which indicated that the cross-reactivity of HC2 might be useful for the detection of the cervical cancer and precancers to some extent. This is perhaps not surprising as many cross-reactive genotypes were probably or possibly carcinogenic, i.e., HPV82, 69, or 53 [15].
In addition to cross-reactivity by HC2, we noticed an extremely low risk of developing CIN2+ for those HC2 negative but LiPA-carcinogenic HPV positive women, which indirectly coincided with the overall good assurance of HC2 against cervical cancer screening [30]. Considering the positive cutoff point for HC2 at 1 pg/mL (signifying at least 5,000 viral copies), this finding corroborated other previous studies that HPV viral copies (viral loads) and carcinogenicity of genotypes were 2 concurrent essential risk factors for the progression to high-grade cervical lesions [2526]. Interestingly, 9.2% women negative by any HPV types by LiPA but HC2 positive were also at a low risk of CIN2+ within subsequent 10 years in our study. Although it remained uncertain whether other types not detected by LiPA caused cross-reactivity and led to false positive rate to some extent, this additional finding indicated these small fractions of HC2 positive women might cause unnecessary referral to colposcopy and reduce the specificity of detecting high-grade cervical lesions. Given more preference attached to sensitivity than specificity on HPV testing, specific biomarkers were required to preclude them from referral or further follow-up. Besides, we confirmed that a HC2 negative test could provide enough assurance against cervical cancer and precancer at least ten years, which were consistent with other publications [272829].
There are several limitations in our study. Primarily, we randomly selected a small fraction of HC2 negative specimens for HPV genotyping using the SPF10-LiPA system, which might lead to selection bias and reduce clinical specificity to CIN2+. However, our focus was to evaluate the long-term risk of women with discrepant assay results, our conclusions would not be influenced to some extent. Secondly, a validation study on specimens with discordant results should be conducted, i.e., using such accurate technology as HPV genome sequencing, which may provide more definite genotyping information. Finally, few CIN3 and cancer cases were identified over the course of 10-year follow-up for analysis of long-term CIN3+ risk even though this population-based cohort was established in a high prevalent area of cervical cancer because women were recommended for treatment immediately after CIN2+ were diagnosed.
In conclusion, based on a prospective cervical cancer cohort, we demonstrated that a HC2 positive result predicted high risk of developing cervical cancer and precancers, even though cross-reacted with untargeted HPV types. Meanwhile a HC2 negative test provided enough assurance against subsequent cervical cancer and precancers. These findings verified the good clinical performance of HC2 in cervical cancer screening.
 XML Download
XML Download