

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pelvic lymph node dissection (PLND) remains an important surgical procedure in patients undergoing radical hysterectomy for cervical cancer. Although the lymph node status is not included in the current International Federation of Gynecology and Obstetrics (FIGO) staging system [1], lymph node metastasis is considered to be an important prognostic factor [234]. However, PLND may be associated with many complications, including vascular and nerve injury, increased blood loss, longer surgery, lymphocyst formation, deep venous thromboembolism, and lower limb lymphedema [5678]. To avoid the complications associated with systematic PLND, the sentinel lymph node (SLN) concept has been applied to the treatment of cervical cancer. The SLN mapping technique is based on the principle that the first nodal group receiving lymphatic drainage from a primary tumor can be identified. The utility of SLN mapping has been well established in melanoma, breast cancer, and vulvar cancer [91011]. Confirmation of this concept brings benefits to cervical cancer patients. When an SLN can be intraoperatively diagnosed using frozen sections, systematic PLND may be omitted. After SLN mapping and a detailed examination of the SLN, micrometastasis may be found; these patients may receive adjuvant therapy. The National Comprehensive Cancer Network (NCCN) cervical cancer guideline presents SLN mapping as an alternative for the surgical management of early-stage cervical cancer less than 2 cm in diameter [12].
Recently, new therapeutic approaches, such as neoadjuvant chemotherapy (NAC) and laparoscopic surgery, for the primary treatment of uterine cervical cancer have been proposed. NAC followed by radical hysterectomy has been proposed to diminish the expansion of tumors and eliminate distant metastasis for locally advanced cervical cancer [1314151617]. Laparoscopic radical hysterectomy has also recently been developed for early-stage cervical cancer following its initial introduction in 1992 [1819]. However, few studies have so far examined the SLN detection rates among different surgical procedures (such as open surgery or laparoscopic surgery) or the influence of pre-surgical treatment (such as diagnostic cervical conization or NAC) on the outcomes of patients with uterine cervical cancer, and the most suitable tracer and the indications for uterine cervical cancer have not been standardized.
In the present study, we assessed the feasibility and diagnostic accuracy of SLN detection in patients with cervical cancer, including patients who have undergone laparoscopic surgery or NAC.
MATERIALS AND METHODS
1. Participants
Between September 2012 and May 2016, a total of 119 Japanese cervical cancer patients underwent a sentinel node procedure at Osaka Medical College in Japan. All of the patients underwent laparoscopic or abdominal radical hysterectomy with or without bilateral salpingo-oophorectomy (BSO) or PLND. The present study was approved by the institutional review board and the participants gave their informed consent.
2. The SLN mapping procedure
All of the tracers were sub-mucosally injected in four quadrants of the cervix at 0, 3, 6, and 9 o’clock. The cervical injection was about 5 mm in all cases, as described previously [2021]. On the day before the operation, 2.0 mL of fluid containing 110 MBq 99m-technetium (99mTc)-labeled tin colloids was injected into the patient’s cervix. Lymphoscintigraphy was performed within 6 hours, and hot spots, indicating SLNs, were identified. On the day of the operation, 5 mL of indigocarmine (IDC) (4 mg/mL) and/or indocyanine green (ICG) (50 µg/mL) was injected into the cervix at the start of surgery. SLN was detected at 40 minutes after injection of IDC or ICG. Radioactive lymph nodes were located using a gamma-probe (Navigator GPS; RMD Instruments Inc., Watertown, MA, USA). IDC-stained lymph nodes were detected by direct inspection. ICG fluorescence-positive lymph nodes were detected using a color fluorescence camera (Hyper Eye Medical System; MIZUHO Medical Co., Ltd., Tokyo, Japan, for laparotomy; Camera Control Unit JC300; MC Medical Co., Tokyo, Japan, for laparoscopy). After SLN biopsy, the area of pelvic lymph node was surveyed by direct observation, and with a color fluorescence camera or a gamma-probe to confirm that no radioactive tissue remained. The combination of 99mTc and IDC was used in early phase and combination of three tracers were used in late phase.
3. Pathology and SLN analyses
An intraoperative pathological examination was performed. The SLN was cut in half, parallel to the longest axis to obtain a maximal section area. One was used to create a frozen section. The specimen was cut with an interval of 2 mm and a 5 µm section, which was stained with hematoxylin and eosin (H&E), was evaluated at the time that the frozen section was created. The other half and the non-SLN specimens were fixed in 10% formalin for a permanent section procedure; the specimen was cut parallel to the longest axis with an interval of 2 mm. After fixation, the 5 µm-thick sections were stained with H&E and examined.
4. Detection rate, sensitivity, and false negative rate
Fig. 1 shows the calculations of the sensitivity, false negative (FN) rate, and negative predictive value in the study participants. The calculations of each rate were side-specific. The detection rate was defined as the ratio of the number of sides with at least one detected SLN to all sides. The sensitivity was defined as the ratio of the number of sides with at least one involved SLN to the number of sides with at least one involved node among the sides with at least one detected SLN. A FN was defined as ipsilateral pelvic lymph node metastasis without SLN metastasis; the FN rate was defined as the ratio of the number of sides with a FN case of SLN biopsy to the number of patients with at least one involved node, SLN or not, among sides with at least one detected SLN.
Fig. 1
The calculations of the sensitivity, false negative (FN) rate, and negative predictive value in the study participants. The calculations of each rate were side-specific. Among all 119 patients, 116 had systematic pelvic lymph node dissection (PLND). Among these patients, sentinel lymph nodes (SLNs) were detected in 189 sides. Metastasis was identified in 22 SLNs, whereas no metastasis was identified in 167 SLNs. However, 9 metastases were identified in the ipsilateral lymph nodes in 167 sides with no SLN metastasis (FN rate, 9/167). No metastases were identified in the ipsilateral nodes in the remaining 158 sides (negative predictive value, 158/167). Among the 31 sides with metastatic lymph nodes, 22 SLNs had metastasis (sensitivity, 22/31). The detection rate was calculated in a total of 119 patients with 238 sides. The sensitivity and FN rate were calculated in the 116 patients who underwent systematic PLND and 189 sides with detected SLNs. The total detection rate, sensitivity, and FN rate were 81.9% (195/238), 71.0% (22/31), and 5.4% (9/167), respectively.

5. Statistical analysis
Each rate including the detection rate, sensitivity, and FN rate, was calculated according to the side. All of the statistical analyses were performed using the JMP software package (version 11.1.1; SAS Institute Inc., Cary, NC, USA). Continuous variables are expressed as the mean±standard deviation (SD). The Mann-Whitney U-test was used to compare continuous variables, and Fisher’s exact test was used to compare frequencies. p values of <0.05 were considered to indicate statistical significance.
RESULTS
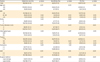
Table 1 shows the characteristics of 119 patients with uterine cervical cancer who underwent SLN biopsy. The mean age of the patients was 46.0 years, and the mean body mass index (BMI) was 22.5 kg/m2. Forty-one (34.5%) patients were nulliparous. A total of 18 patients had FIGO stage IA disease, 50 had stage IB1 disease, 5 had stage IB2 disease, 9 had stage IIA1 disease, 10 had stage IIA2 disease, and 23 had stage IIB disease. Histologically, 74 patients had squamous cell carcinoma and 45 had adenocarcinoma. The SLN procedure was performed with 99mTc in 106 (89.1%) patients, IDC in 114 (95.8%) patients, and ICG in 43 (36.1%) patients. Forty-three (36.1%) of the patients had a history of cervical conization and 28 (23.5%) received neoadjuvant intra-arterial chemotherapy (NAIC). The mean tumor size before and after NAC was 4.3±1.2 and 1.4±1.6 cm, respectively. Twenty-five (21.0%) patients underwent laparoscopic surgery; 94 (79.0%) patients underwent laparotomy. A total of 116 (97.5%) patients underwent systematic PLND after SLN biopsy. The mean number of detected SLNs was 2.7±2.0. The total number of resected lymph nodes was 37.4±11.9. Fig. 1 shows the calculation of the sensitivity, FN, and negative predictive value in the study participants. The calculations of each rate were side-specific. Among all 119 patients, 116 had systematic PLND. Among these patients, SLNs were detected in 189 sides. Metastasis was identified in 22 SLNs, whereas no metastasis was identified in 167 SLNs. However, 9 metastases were identified in the ipsilateral lymph nodes in 167 sides with no SLN metastasis (FN rate, 9/167). No metastases were identified in the ipsilateral nodes in the remaining 158 sides (negative predictive value, 158/167). Among the 31 sides with metastatic lymph nodes, 22 SLNs had metastasis (sensitivity, 22/31). Table 2 shows the associations between the detection rate, sensitivity, and FN rate and the related factors. The total detection rate, sensitivity, and FN rate were 81.9% (195/238), 71.0% (22/31), and 5.4% (9/167), respectively. Elderly patients (≥60 years of age) had a lower detection rate than younger patients (<60 years) (65.8% vs. 85.0%, p<0.01). The sensitivity and FN rate did not differ to a statistically significant extent (sensitivity, 57.1% vs. 75.0%, p=0.3; FN, 14.3% vs. 4.1%, p=0.1). The findings for the severely obese (BMI ≥30 kg/m2), moderately obese (BMI 25–30 kg/m2), and non-obese (BMI <25 kg/m2) patients did not differ to a statistically significant extent (detection rate, 93.8% vs. 80.4% vs. 81.2%, p=0.2, p=0.9; sensitivity, 75% vs. 50% vs. 72.0%, p=0.9, p=0.5; FN, 8.3% vs. 3.6% vs. 5.5%, p=0.7, p=0.7, respectively). There was no significant difference between nulliparous and multiparous patients (detection rate, 84.2% vs. 80.8%, p=0.5; sensitivity, 71.4% vs. 70.8%, p=0.6; FN, 3.2% vs. 6.7%, p=0.4). The patients with ≥2-cm-diameter tumors had a lower detection rate (75.7% vs. 91.5%, p<0.01) and a higher FN rate (8.6% vs. 1.4%, p<0.01) than the patients with <2-cm-tumors. Although having a ≥2-cm-diametertumor was associated with lower sensitivity, the difference was not statistically significant (66.7% vs. 85.7%, p=0.4). There was no statistically significant difference between the patients with squamous cell carcinoma and adenocarcinoma (detection rate, 81.8% vs. 82.2%, p=0.9; sensitivity, 71.4% vs. 70.0%, p=1.0; FN, 6.0% vs. 4.5%, p=0.7). 99mTc had a higher detection rate than IDC and ICG (85.8% vs. 20.2% and 61.6%, p<0.01). Among the patients without NAC, 99mTc also had a higher detection rate than IDC and ICG (90.6% vs. 22.4% and 75.9%, p<0.01). The sensitivity and FN rates of the tracers did not differ to a statistically significant extent. The sensitivity was higher in the patients with history of conization than those without that (91.4% vs. 78.0%, p=0.02). The sensitivity and FN of the patients with and without a history of conization did not differ to a statistically significant extent (sensitivity, 80.0% vs. 69.2%, p=1.0; FN, 1.9% vs. 7.1%, p=0.1). The patients with NAC had a lower detection rate (67.9% vs. 86.3%, p<0.01) and a higher FN rate (19.4% vs. 2.2%, p<0.01) than those without NAC. The patients with NAC had lower sensitivity; however, the difference was not statistically significant (53.9% vs. 83.3%, p=0.1). The patients who underwent a laparoscopic procedure had a higher detection rate (100.0% vs. 77.1%, p<0.01) and lower FN rate (0% vs. 7.4%, p<0.01) than those with laparotomy. The sensitivity did not differ to a statistically significant extent (100.0% vs. 66.7%, p=0.3). Six of the 23 SLNs with metastasis (26.1%) could not be diagnosed using intraoperative frozen sections.
Table 1
The characteristics of the patients with cervical cancer who underwent a SLN biopsy

Table 2
The detection rate, sensitivity and FN rate of SLNs in cervical cancer
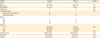
Next, we evaluated the diagnostic accuracy SLN biopsy specimens obtained from patients with laparoscopy or NAC. The diagnostic accuracy was evaluated in patients with non-bulky cervical cancer (<4 cm in diameter) who underwent laparoscopy and laparotomy, because laparoscopic surgery is not performed to the patients with bulky tumors in our institution. Table 3 compares the results of laparoscopy and laparotomy in patients with stage IA, IB1, and IIA1 cervical cancer. The age, BMI, proportion of nulliparous patients, and histological types were not significantly different. The patients who underwent laparoscopic procedures had a higher rate of ICG use and a lower rate of IDC use than patients who underwent laparotomy; however, the rate of 99mTc use did not differ to a statistically significant extent. More of the patients in the laparotomy group had a history of conization (32.0% vs. 46.2%, p=0.04). Laparoscopic procedures were associated with a higher detection rate than laparotomy (100.0% vs. 87.5%, p<0.01); however, the sensitivity and FN rate were not significantly different (sensitivity, 100.0% vs. 83.3%, p=0.2; FN, 0.0% vs. 1.3%, p=0.4). The diagnostic accuracy of SLN biopsy was evaluated in patients with bulky tumor (≥4 cm in diameter) who received or did not receive NAC, as NAC is performed patients with bulky tumors in our institution. Table 4 shows the diagnostic accuracy of SLN biopsy in patients with bulky tumors. Among the patients with bulky tumors, the values including detection rate, sensitivity, and FN were not significantly different between the patients with and without NAC.
Table 3
The results of laparoscopy and laparotomy in patients with stage IA, IB1, and IIA1 cervical cancer
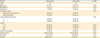
Table 4
The results of NAC in patients with bulky tumors
DISCUSSION
In the current study, 99mTc had the highest detection rate of the three tracers. In contrast, the use of IDC was associated with a low detection rate. The patients with advanced disease and NAC had unfavorable detection and FN rates. In contrast, laparoscopic procedures were associated with especially favorable figures in patients with early-stage disease. Several factors, including BMI, parity, histological type, and a history of conization had no significant impact on the detection rate, sensitivity or FN rate.
A meta-analysis showed that the SLN detection rate in cervical cancer was 89.2%–93.0% [222324]. The detection rates with blue dye, the isotope and a combination of both tracers were 80.9%–87.5%, 90.0%–90.9%, and 92.3%–97.0%, respectively. Although one author concluded that there were no significant differences between the tracers, others did not. IDC was used as the blue dye tracer in the current study. In Japan, SLN biopsy using IDC has been performed since 1998, mainly in breast cancer [25]. Its molecular mass is 466.4, which is similar to patent blue and isosulfan blue; however, the detection rate using IDC was extremely low in the current study. In contrast, ICG (a fluorescent dye) has a molecular mass of 775. Although SLN biopsy using ICG requires a fluorescence system, several reports have shown that ICG has a feasible detection rate in patients with uterine cervical cancer [262728]. On the other hand, in the patients with uterine cervical cancer, the sensitivity of radiotracers has been reported to be 87.0%–94.4% [222324]. The use of a radiotracer in combination with blue dye did not increase the sensitivity to a significant extent (88.0%–91.3%). Similarly, blue dye used alone did not decrease the sensitivity to a significant extent (86.3%–87.2%) [222324]. The sensitivity with fluorescent imaging was 90.9% [24]. Based on the results of the current study, we believe that SLN biopsy using a radiotracer is the most useful method of SLN detection in patients with uterine cervical cancer.
A large tumor size and an advanced stage were associated with lower detection rate and sensitivity [24]. The detection rate and sensitivity were lower in the patients with advanced-stage cancer (>IB2) than in patients with early-stage cancer (≤IB2) (detection rate, 65.9% vs. 93.6%; sensitivity, 87% vs. 91.4%) [24]. Similarly, the detection rate and sensitivity were lower in patients with large-sized tumors (>2 cm) than in those with small tumors (≤2 cm) (detection rate, 73.9% vs. 93.4%; sensitivity, 81.7% vs. 94.7%) [24]. In those patients, the lymphatic tract may be destroyed and the rate of lymph node metastasis is higher. In such cases, non-involved lymph nodes may be detected as SLNs, because the original SLN is completely replaced with cancer cells [29]. The reason for the failure of lymphatic mapping in large or locally advanced tumors is the higher possibility of lymph nodal involvement and lymphovascular invasion, which hampers lymphatic flow, than with smaller tumors [24]. NAC followed by radical hysterectomy has been proposed to diminish the expansion of tumors and eliminate distant metastasis for locally advanced cervical cancer [1314151617]. In this study, the patients with NAC had a lower detection rate (67.9% vs. 86.3%, p<0.01) and a higher FN rate (19.4% vs. 2.2%, p<0.01) than those without NAC, as found in a previous report [24]. Basically, preoperative treatment is administered to cervical cancer patients who have bulky tumors [13]. NAC might be associated with a better detection rate due to the regression of the tumor in the lymphatic drainage or lymph nodes. However, the detection rate among the patients with bulky tumors was not significantly different between the patients with and without NAC in our study (68% vs. 60%, p=0.4). Some prominent findings after NAC treatment were elastosis, collageniztion, hyalinaization, and microcalicification of the stroma; hyalinization of the walls of the blood vessels; and necrosis [30]. These changes suggest that NAC might induce blocking or rerouting of the lymphatic drainage of the primary tumor. Our data further suggest that the unfavorable results after NAC were caused by not only the presence of large and advanced tumors but also the chemotherapy itself. We believe that patients who have received NAC for locally advanced cervical cancer might be unsuitable for SLN mapping.
The injection of tracers to patients with a history of conization is difficult and conization may hamper lymphatic flow. However, in line with the results of a previous study, we found that a history of conization was not associated with a lower detection rate [24].
The detection rates in patients who underwent laparoscopic surgery and open surgery were 93.0%–96.1% and 87.0%–90.2%, respectively. The sensitivity in these patients was 89.8%–93.2% and 86.0%–91.7%, respectively [222324]. These results suggest that laparoscopic procedures have excellent potential in detecting SLNs in patients with early cervical cancer. In our study, laparoscopic procedure had higher detection rate than laparotomy. We believe that a wide and clear view by laparoscopy improves the detection rate; in more patients with higher detection rate under laparoscopy, systematic PLND could be omitted.
This study is associated with two important limitations that may potentially decrease its value. First, a multivariate analysis could not be performed due to the small study size. Second, the study included a number of biases. For example, most of the patients who received NAC had advanced disease. Similarly, most of the patients with a history of conization or those who underwent a laparoscopic procedure had early disease. In this point of view, the conclusion is not definitive.
In conclusion, 99mTc had the highest detection rate of the three tracers. The patients with advanced-stage cancer and those who received NAC had an unfavorable detection rate and FN. In contrast laparoscopic surgery was associated with a favorable detection rate and FN, especially in patients with early-stage disease. To avoid systematic PLND, SLN biopsy should be performed during laparoscopic surgery in patients with early-stage disease. Laparoscopic devices may be useful for this SLN procedure.
 XML Download
XML Download