

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute appendicitis is the most common cause of acute abdominal pain requiring surgery. The most important complication of appendicitis is appendiceal perforation, which is associated with serious morbidities and even mortality [1].
Clear definition of appendiceal perforation has several clinical implications. First, appendiceal perforation rate (the proportion of perforation cases out of all appendicitis cases), together with negative appendectomy rate (the proportion of removal of noninflamed appendices out of all appendectomies), has been traditionally regarded as an important metric for the quality of care in patients with suspected appendicitis [2]. Although several studies [3] questioned the relevance of appendiceal perforation rate as a quality metric by suggesting that most perforations occur before patient hospital visit, this debate does not essentially diminish the importance of clear definition of perforation. Second, appendiceal perforation rate has been also used as a surrogate index for the quality of general acute care in studies measuring ethnic and socioeconomic disparities [45]. Third, preoperative knowledge of appendiceal perforation can critically alter the treatment plan. Several randomized controlled trials [67] have recently suggested the feasibility of nonoperative treatment for appendicitis. For such nonoperative treatment to be truly successful, it is important to preoperatively discriminate uncomplicated appendicitis cases from perforated or gangrenous cases. In addition, perforated appendicitis is a relative contraindication for minimally invasive appendectomy procedures particularly at the hand of less experienced surgeons [89], due to the risk of postoperative intraabdominal abscess formation, although experienced surgeons would more accept laparoscopic approach regardless of the presence of perforation.
However, the definition of appendiceal perforation has surprisingly been missing or inconsistent in many of previous studies addressing appendiceal perforation rate [5] or preoperative diagnoses of appendicitis [10]. The ambiguity may partly explain the wide range of reported appendiceal perforation rates (16%–39%) as summarized by Birnbaum and Wilson [11]. St Peter et al. [12] even stated that “all retrospective data published on perforated appendicitis are unreliable” because of the poor definition of perforation. In particular, previous studies have rarely clarified whether appendiceal perforation indicated gross perforation with periappendiceal abscess or generalized peritonitis, or included also microperforation with localized peritonitis of minimal extent. While the former can be identified during surgery, the latter is likely identifiable only via microscopic examination of the appendectomy specimen [1314]. We hypothesized that the former is associated with the surgical approach or with the patient's prognosis, while the latter is not so.
The purpose of this study was to retrospectively determine whether appendiceal perforation identified pathologically but not surgically is associated with the use of laparoscopic appendectomy or with the length of hospital stay in adolescents and young adults, and to establish a clinically meaningful reference standard for appendiceal perforation for future studies addressing appendiceal perforation rate or preoperative diagnosis of appendiceal perforation.
METHODS
Study overview
The Institutional Review Boards of all investigating sites (Bundang Jesaeng General Hospital, Myongji Hospital, Hanyang University Hospital, Hallym University Kangnam Sacred Heart Hospital, Seoul National University Bundang Hospital, Soonchunhyang University Seoul Hospital, Soonchunhyang University Bucheon Hospital, Samsung Medical Center, Korea University Guro Hospital, Hallym University Sacred Heart Hospital, and Korea University Ansan Hospital) approved this study (Supplementary Table 1) and waived patient informed consent for review of patients' medical records. Our study had 2 components. First, to reveal the ambiguity in the definition of appendiceal perforation in previous studies, we extensively reviewed articles addressing appendiceal perforation published in 2012–2013. Second, we performed a retrospective study including 1,438 adolescents and young adults with confirmed appendicitis in 11 hospitals in 2011. The patients were classified as follows: nonperforation (group 1), perforation identified pathologically but not surgically (group 2), perforation identified surgically but not pathologically (group 3), and perforation identified both pathologically and surgically (group 4). We compared the 4 groups in terms of the use of laparoscopic appendectomy and the length of hospital stay associated with appendectomy.
Literature review
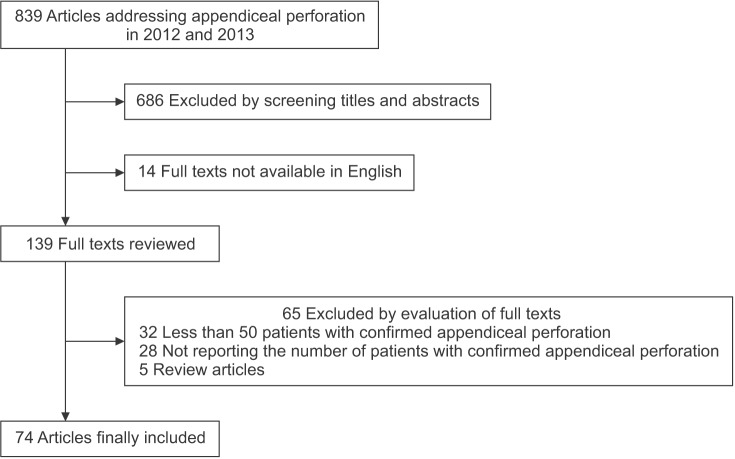
Two radiologists (with 12 and 14 years of experience, respectively) and 1 epidemiologist jointly searched the MEDLINE database (Supplementary Table 2) and identified 839 articles seemingly addressing appendiceal perforation from January 2012 through December 2013. The 2 radiologists reviewed the articles and extracted the data. Their disagreements were resolved by consensus. By screening the titles and abstracts, the radiologists excluded 686 articles. Fourteen additional articles were excluded because the full texts were not available in English. After reviewing the full texts, 65 articles were further excluded because they included less than 50 patients with confirmed appendiceal perforation (n = 32), did not report the number of patients with confirmed appendiceal perforation (n = 28), or were review articles (n = 5). The remaining 74 articles were finally included in our literature review (Fig. 1, Supplementary Table 3). The two radiologists extracted the following information: name of the first author, number of subjects with appendiceal perforations, number of subjects with confirmed appendicitis, appendiceal perforation rate, standard of reference for appendiceal perforation, and descriptor defining appendiceal perforation.
Retrospective study
Database
The data in our retrospective study were extracted from a database of a recent cross-sectional study [15] aimed at measuring the computed tomography utilization rate and negative appendectomy rate in patients with appendicitis in metropolitan Seoul, Korea, which was conducted by the Low-dOse Computed Tomography for Appendicitis Trial (LOCAT) group. The database included adolescents and adults undergoing nonincidental appendectomy in 2011 at 11 hospitals in metropolitan Seoul. Data were collected from medical records as well as from questionnaires and interviews of site investigators by 2 study coordinators (2 radiologists with 1 and 13 years of experience, respectively) in conjunction with site investigators from November 2012 through April 2013. Eight tertiary and 3 secondary hospitals with a median bed number of 800 (range, 554–1,950) participated in the formation of the database (Supplementary Table 1). All hospitals were located in metropolitan Seoul, and accounted for 18% of the 63 hospitals having 300 or more beds in metropolitan Seoul [16] where 40,000 appendectomies are performed annually from a total population of 21 million [17] . The site investigators searched hospital information systems to identify patients who visited the Emergency Departments and then underwent appendectomy, cecectomy, or ileocecectomy. In this study, cecectomy and ileocecectomy as well as simple appendectomy performed were collectively termed nonincidental appendectomy, if the surgical procedure was aimed at the treatment of presumptive appendicitis. In all sites, appendectomy was the treatment of choice for appendicitis. None of the site attempted non-operative treatment for appendicitis during the study period.
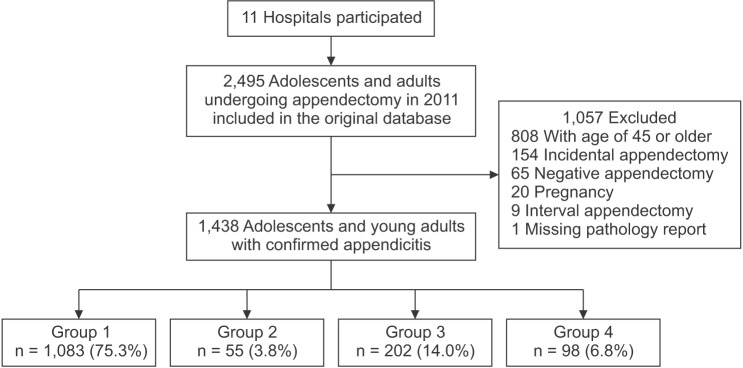
The database included 2,495 consecutive patients aged 15 years or older who underwent appendectomy. We excluded cases of 45 years or older (n = 808), incidental appendectomy (n = 154), negative appendectomy (n = 65), pregnancy (n = 20), interval appendectomy following percutaneous abscess drainage (n = 9), or missing pathology report (n = 1). The presence of appendicitis was based on clear documentation of appendicitis or neutrophil infiltration in the appendiceal wall in pathology reports [18]. If neutrophilic collection is confined to the mucosa, the diagnosis was based on the documentation of mucosal ulcerations [19]. We empirically chose the lower age threshold of 15 years, reflecting the typical practice pattern of the 11 sites in grouping patient age for choosing imaging study for suspected appendicitis. We excluded the older patients, with an arbitrary threshold of 45 years, because the database had limited information on their comorbidities, which could be important confounders or effect modifiers of the study hypothesis [20]. Therefore, our retrospective study finally included the remaining 1,438 adolescents and young adults (mean age, 29.3 ± 8.4 years; 785 men [29.2 ± 8.7 years] and 653 women [29.3 ± 8.2 years]) with confirmed appendicitis (Fig. 2). They were deemed as rarely having serious comorbidities. According to the pathologic reports, the study sample included 22 patients with appendiceal diverticulitis and four with appendiceal neoplasms, which were complicated by appendicitis. The study sample accounted for 6.2% of total appendectomies in patients 15–44 years of age in the metropolitan Seoul in the same period [17].
Appendiceal perforation
Two radiologists classified the 1,438 patients into groups 1–4 according to the surgical or pathologic documentations of appendiceal perforation. Pathologically identified perforation was defined as a clear documentation of perforation or observation of an appendiceal wall defect due to transmural necrosis [1314] in pathologic reports based on either gross examination of the specimen or histopathological examination of tissue sections. Surgically identified perforation was defined as a clear documentation of perforation, or observation of spilled appendiceal contents, abscess, obvious peritonitis, or appendiceal wall defect in surgical records [21]. If there was no clear mention of perforation in the pathologic report or surgical record, the patient was regarded as not having pathologically or surgically identified perforation, respectively.
Endpoints
The retrospective study had 2 endpoints: the use of laparoscopic appendectomy and the length of hospital stay. The former is an important issue in surgical planning [8] and the latter is an important outcome measure in patients undergoing appendectomy [22]. Small number of open conversions following initial laparoscopic approach were counted as open appendectomies. The length of hospital stay was defined as the interval from the induction of anesthesia for appendectomy to hospital discharge. A prolonged hospital stay was defined as 3.7 days (89 hours) or longer with the threshold based on the 75th percentile value in group 1 [23].
Statistical analysis
The number of patients eligible for the present study determined the sample size. All analyses were planned after the formation of the original study database [15] but before the selection of the present study sample. The chi-square tests were used for the comparison of baseline characteristics among the four groups.
The 4 groups were compared for the use of laparoscopic appendectomy using the Bonferroni adjustment and for the length of hospital stay using the Kruskal-Wallis test with post hoc Dunn pairwise comparisons. Multivariable as well as univariable logistic regression analyses were performed to determine the association between the 4 groups and the use of laparoscopic appendectomy or the length of hospital stay. Covariates included age, sex, body mass index, time of presentation at the emergency department, time to appendectomy, and mode of surgical approach [24]. Generalized estimating equations were used to adjust for clustering effects by site, and thereby to prevent an inflation of type I error. The use of the generalized estimating equations would help to estimate the average trend across the sites by taking into consideration the site heterogeneity. Nine cases with missing data in body mass index were not included in the multivariable analyses. P-values less than 0.05 were considered statistically significant. Statistical analyses were performed using Stata ver. 13.0 (StataCorp LP., College Station, TX, USA).
RESULTS
Literature review
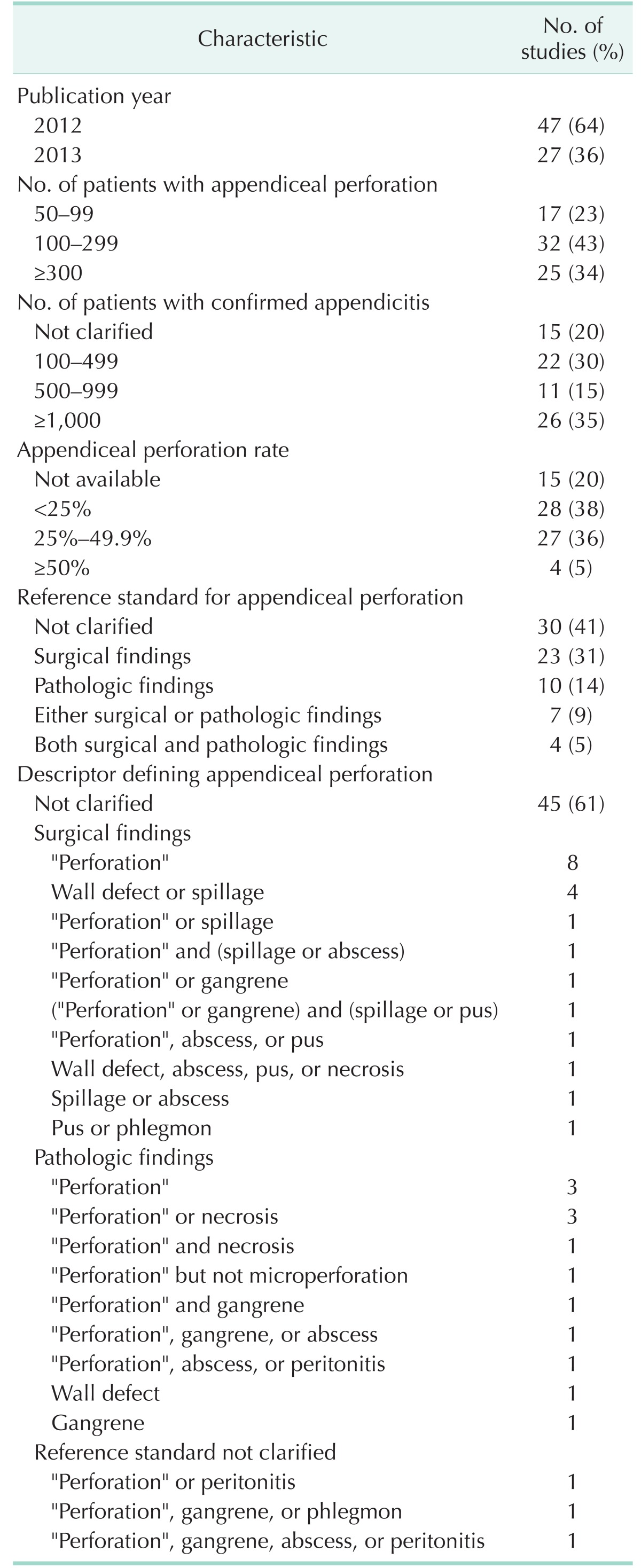
The results of the 74 selected studies are summarized in Table 1. Twenty-five studies (34%) used International Classification of Disease code-9 or -10 for the patient inclusion. Thirty studies (41%) did not clarify the reference standard for appendiceal perforation. Of the remaining 44 studies, 23 (31%), 10 (14%), 7 (9%), and 4 (5%) used surgical, pathologic, either surgical or pathologic, and both surgical and pathologic findings, respectively, as the reference standard.
The reported appendiceal perforation rate ranged from 5.8% to 62% in 59 of the 74 included studies. In the remaining 15 studies, appendiceal perforation rate was not reported or could not be calculated from the reported data. In the studies using surgical, pathologic, and either surgical or pathologic findings as the reference standard, appendiceal perforation rate range was 13.2%–62%, 8.5%–38.6%, and 13.7%–60.5%, respectively.
Forty-five of the 74 studies (61%) did not clarify the descriptor defining appendiceal perforation. In the remaining 29 studies, a variety of descriptors were used (Supplementary Table 3). For the surgical or pathologic definition of appendiceal perforation, 10 studies used “perforation” as the sole descriptor without further clarification and 16 studies used “perforation” as one of the descriptors.
Appendiceal perforation
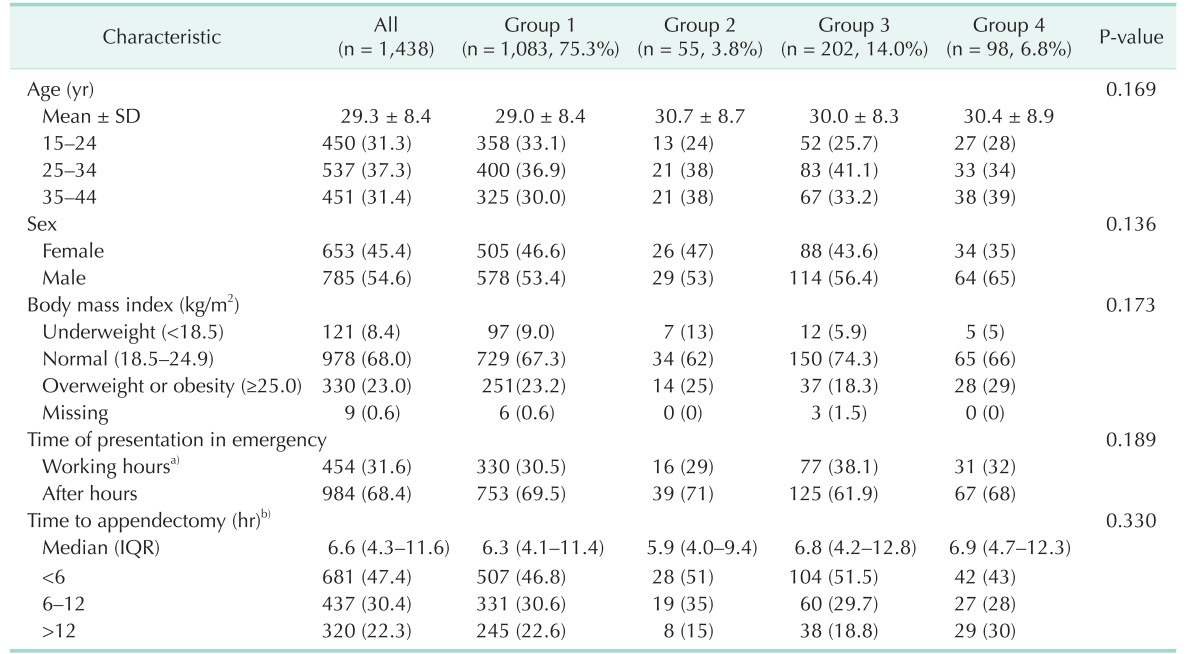
Of the 1,438 patients included in the study, 1,083 (75.3%), 55 (3.8%), 202 (14.0%), and 98 (6.8%) were classified into groups 1–4, respectively (Table 2). Overall, 355 (24.7%) had perforation documented in pathologic reports or surgical records. Fifteen patients had to undergo cecectomy (n = 12) or ileocecectomy (n = 3) instead of simple appendectomy for the following reasons. In 14 patients who were classified into groups 3 (n = 4) and 4 (n = 10), the surgeons considered the inflammation was too extensive to be treated with simple appendectomy. In 1 patient who was classified into groups 2, the surgeon chose to convert to cecectomy due to severe cecal edema and adhesion.
Use of laparoscopic appendectomy
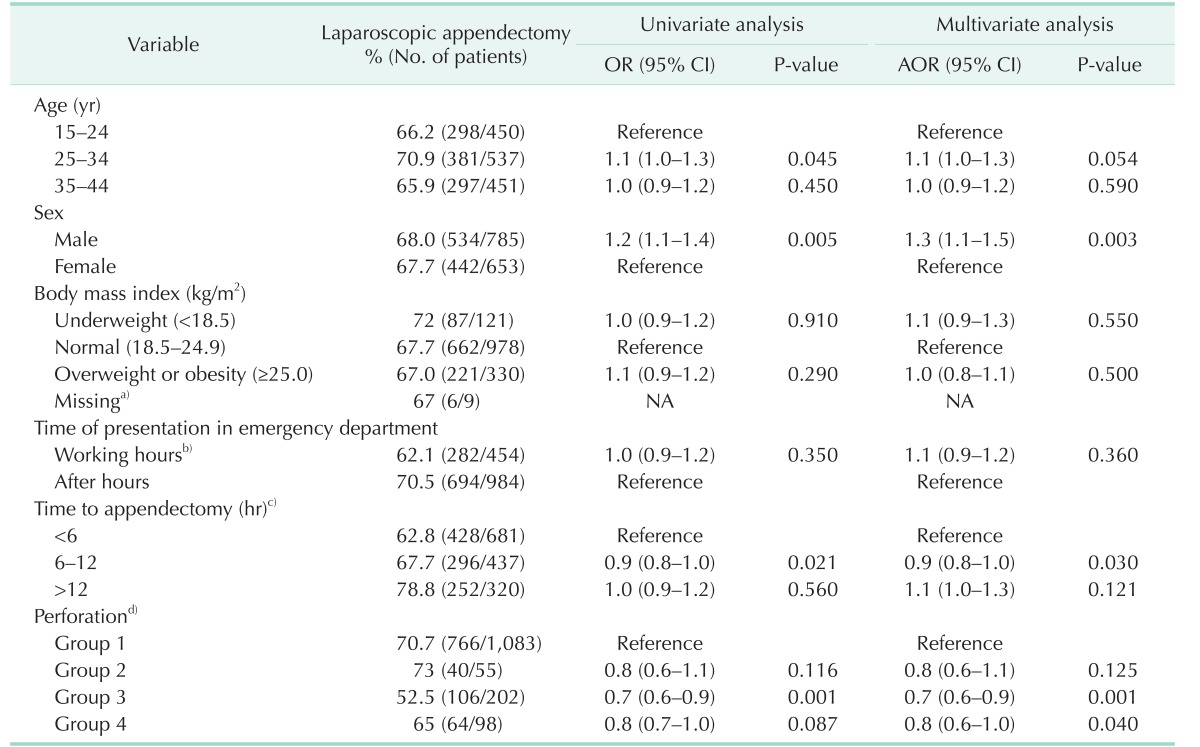
Overall, the laparoscopic approach was used in 976 of the 1,438 patients (67.9%); this included 70.7% (766 of 1,083), 73% (40 of 55), 52.5% (106 of 202), and 65% (64 of 98) of the patients in groups 1–4, respectively. Using the Bonferroni adjustment, group 1 significantly differed from group 3 (P < 0.001) but not from group 2 (P = 0.871) or 4 (P = 0.310). No significant differences were observed for the remaining pairwise comparisons (P = 0.010–0.450). The data for each investigating site are available in the Supplementary Table 4.
In the univariable logistic regression analyses, group 3 was significantly associated with lower use of laparoscopic appendectomy. Age (25–34 years), male, and time to appendectomy (6–12 hours) were significantly associated with higher use; however, the differences between the subgroups were small (Table 3). In the multivariable analysis adjusted for clustering effects by site, the use of laparoscopic appendectomy was less frequent in groups 3 (adjusted odds ratio [AOR], 0.7; 95% confidence interval [CI], 0.6–0.9; P = 0.001) and 4 (AOR, 0.8; 95% CI, 0.6–1.0; P = 0.040) than in group 1, but was not significantly different between groups 1 and 2 (AOR, 0.8; 95% CI, 0.6–1.1; P = 0.125) (Table 3). The covariates significantly associated with higher use of laparoscopic appendectomy in the multivariable analysis were male and time to appendectomy (6–12 hours). The results of the analyses unadjusted for clustering effects by site are available in the Supplementary Table 5.
Length of hospital stay
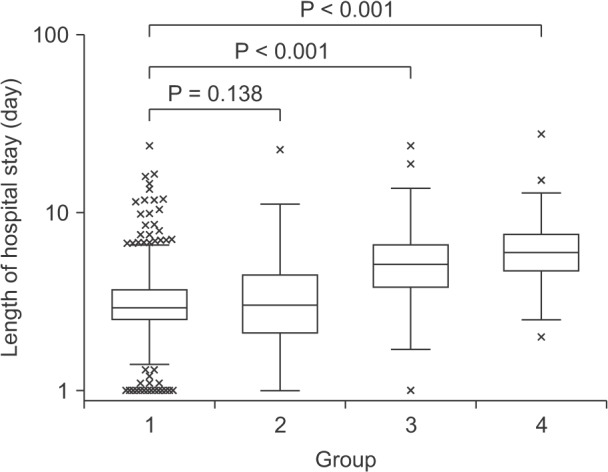
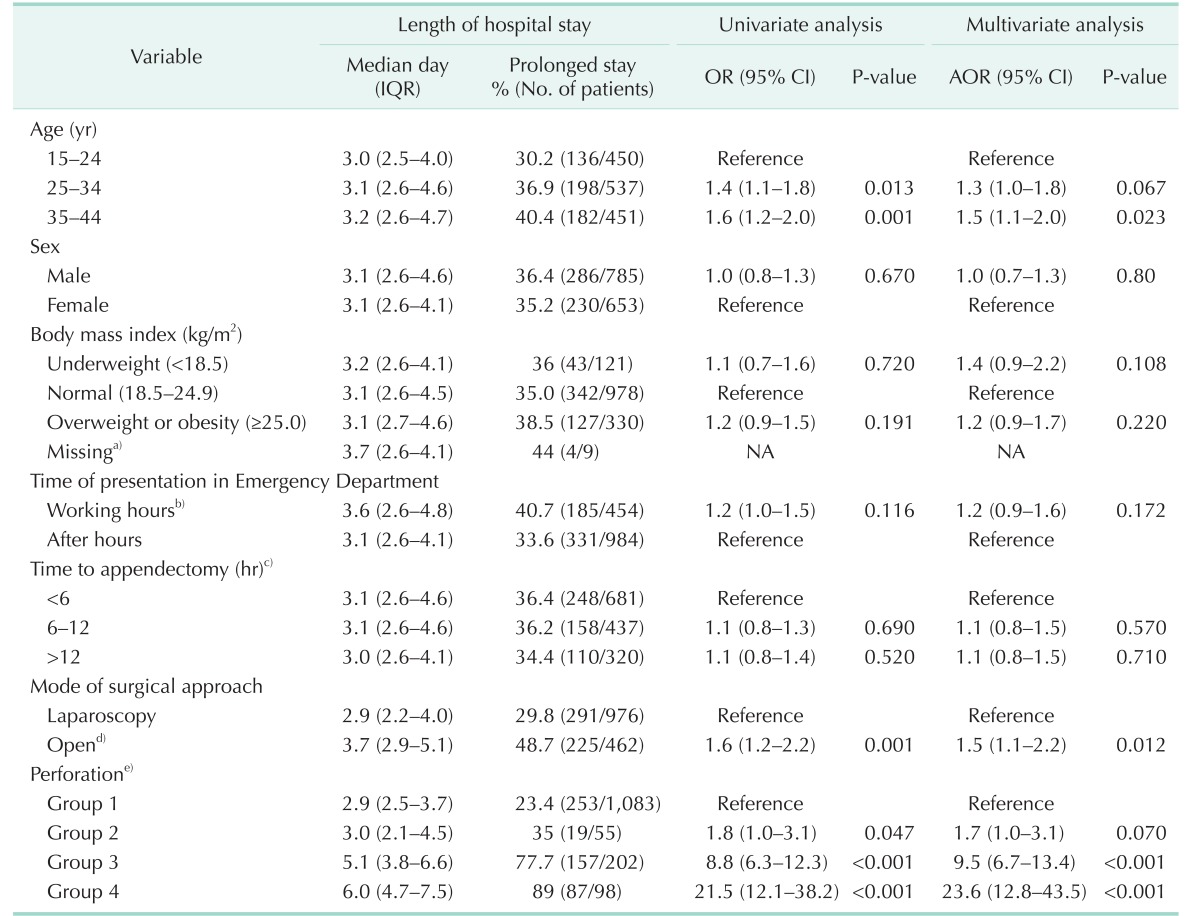
Overall, the median length of hospital stay was 3.1 days (interquartile range, 2.6–4.5 days). The median length of the hospital stay (interquartile range) for groups 1–4 was 2.9 (2.5– 3.7), 3.0 (2.1–4.5), 5.1 (3.8–6.6), and 6.0 days (4.7–7.5 days), respectively (P < 0.001). In the pairwise comparisons, groups 3 and 4 significantly differed from groups 1 or 2 (P = 0.138), whereas no significant difference was observed between groups 1 and 2 (P = 0.138) or groups 3 and 4 (P = 0.068) (Fig. 3). The length of the hospital stay at each investigating site is summarized in the Supplementary Table 6.
In the univariable logistic regression analyses, groups 2–4 and open appendectomy were significantly associated with prolonged hospital stay. Age (25–34 or 35–44 years) was significantly associated with the prolonged hospital stay; however, the differences were small (Table 4). In the multivariable analysis adjusted for clustering effects by site, prolonged hospital stay was more frequent in groups 3 (77.7%; AOR, 9.5; 95% CI, 6.7–13.4; P < 0.001) and 4 (89%; AOR, 23.6; 95% CI, 12.8–43.5; P < 0.001) than in group 1 (23.4%), but was not significantly different between groups 1 and 2 (35%; AOR, 1.7; 95% CI, 1.0–3.1; P = 0.070). The covariates significantly associated with the prolonged hospital stay in the multivariable analysis were age (35–44 years) and open appendectomy. Similar results were found in analyses unadjusted for clustering effects by site (Supplementary Table 7).
DISCUSSION
In our results from the 11 sites, discrepancies often occurred between surgical and pathologic findings in regard to the presence of appendiceal perforation in the individual patients. Of the 1,438 patients included in our study, 55 appendiceal perforations were identified in pathologic examination but not during surgery (group 2), and 202 appendiceal perforations were identified during surgery but not in the pathologic examination (group 3). In determining appendiceal perforation, surgeons' inspections during appendectomy can be limited [19], particularly in cases with extensive inflammation [25]. Pus can be present on the serosal surface of the inflamed appendix even in the absence of perforation, which can result in a false-positive confirmation of perforation [25]. On the other hand, pathologic evaluation can be often limited in demonstrating appendiceal perforation which was evident during surgery [12]. This can be partly attributable to the fact that microscopic examination may miss tiny perforations not included in tissue samples.
It should be noted that what our data suggests is simple association between “laparoscopic approach” and “surgically identified perforation” as surgical identification of appendiceal perforation can be established only after the decision as to the use of laparoscopic approach. Our study was not aimed to propose an individualized management plan by the type of appendiceal perforation. Instead, the motivation for our study was to establish a clinically relevant reference standard for appendiceal perforation for future studies addressing appendiceal perforation rate or preoperative diagnosis of appendiceal perforation. From the literature review, we found a profound inconsistency and ambiguity with regard to the reference standard and descriptor of appendiceal perforation in the previous studies. This may partly explain the wide range of appendiceal perforation rates reported in the studies. Without a consistent and clinically-relevant reference standard for perforation, any data on appendiceal perforation rate or on the treatment of perforated appendicitis would not be truly meaningful.
Our results from the 11 sites indicate that surgical findings are more clinically meaningful than pathologic findings as the reference standard, as surgically identified perforation was significantly associated with the less use of laparoscopic appendectomy and associated with longer hospital stay, while pathologically-identified perforation was not so. These results corroborate the hypothesis by St Peter et al. [12] who stated that pathologic evaluation is less useful than surgeons' observation in identifying perforation. Based on our findings, we recommend not counting pathologically-identified perforation cases (group 2 in our study) as appendiceal perforation in an investigation wherein appendiceal perforation is measured as an endpoint as it was originally meant to be. In term of the practice of individual patients, whether or not group 2 is called as perforation should depend on the clinical context.
Some variations may have existed across as well as within the investigating sites in terms of the criteria or descriptor used for surgical or pathologic diagnosis of appendiceal perforation. It has been suggested to use appendiceal wall defect or spilled fecalith as the descriptors defining appendiceal perforation [12], as this definition can sensitively predict the development of postoperative intra-abdominal abscess. On the basis of our literature review and of our experiences from other studies [132627], we recommend that appendiceal perforation should be determined based on the observation of spilled appendiceal contents, abscess, obvious peritonitis, or appendiceal wall defect observed during surgery. Further studies are needed to establish and standardize the descriptors defining appendiceal perforation.
In regard to the use of laparoscopic appendectomy, we found that the regression model specification and the strength of association were changed if the adjustment for the clustering effects was not considered. This implies some intracluster correlation within site and some heterogeneity across the sites. Our results obtained using the generalized estimating equations represent average trends across the sites by accounting for the clustering effects due to the heterogeneity. The rate of laparoscopic appendectomy varied from 25.8% to 98% across the sites. Specifically, 2 sites used laparoscopic approach less frequently than the remaining sites, probably due to limited availability of laparoscopic surgeons and surgeons' reluctance for laparoscopic approach.
In regard to the length of hospital stay, the results of our regression analyses were consistent regardless of the adjustment of the clustering effects. Our results showed that older age and open appendectomy were associated with prolonged hospital stay, corroborating previous study results [28]. The absolute lengths of hospital stay in our results may be longer than those in other countries [29], which may be associated with the generous reimbursement policy of Korean national medical insurance system in regard to hospitalization cost [30].
Our study had limitations. First, the investigating sites were teaching hospitals that voluntarily participated in the original study. It is unclear if our results can be generalized to other hospitals. Second, we empirically chose the age window of 15–44 years for the inclusion of adolescents and young adults. Our results may not be generalized to patients with other ages. Furthermore, other hospitals may use different age thresholds in grouping patient age for choosing imaging study for suspected appendicitis. Third, as our database was originally formed for another study [15], we did not have individual patient data of comorbidities, postoperative complications such as intra-abdominal abscess, or preoperative CT findings.
In conclusion, we found a profound inconsistency and ambiguity with regard to the reference standard and descriptor of appendiceal perforation in the previous studies. Our study of adolescents and young adults with appendicitis shows that surgically identified appendiceal perforation is associated with the less use of laparoscopic appendectomy and with longer hospital stay, while pathologically identified perforation is not so. We recommend using surgical rather than pathologic findings as the reference standard for the presence of appendiceal perforation in future investigations on appendiceal perforation rate or preoperative diagnosis of perforation.
 XML Download
XML Download