

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Korea is rapidly becoming an aging society; it is estimated that the number of people aged over 65, which was 7% of total Korean population on 2002, will reach 20% by 2026 [1]. This tendency is overtaking the global average and if it were to persist, Korean population might surpass Japan by 2040 (Fig. 1)
It is not hard to predict that diseases that commonly affect the old, such as arterial diseases, will increase with time [23]. The epidemiology and treatment of major arterial disease (MAD), including cerebrovascular diseases and coronary arterial diseases, have been studied extensively and are relatively well established [456789]. However, carotid arterial occlusive diseases (CAOD), abdominal aortic diseases (AAA) and arterial diseases of the lower extremities (LAOD) in Korea have been less studied.
This study aims to figure out the changes of the prevalence and management of MAD, including CAOD, AAA, and LAOD in Korea over the past 5 years, and predict future trends.
METHODS
Data for this study were extracted from the Health Insurance Review and Assessment Service (HIRA) during the period from 2008 to 2012. Disease and treatment codes provided by HIRA were assigned to each disease and treatment that fall under the category of MAD (Table 1). We excluded aortic dissections, occlusive diseases of the upper extremities, mesenteric or renal arteries, and all aneurysmal diseases that developed elsewhere but the abdominal aorta.
The HIRA disease classification codes for LAOD were ambiguous, and 5 of 7 codes did not indicate LAOD appropriately. For example, atherosclerosis was divided into 3 subdivisions according to their location in the HIRA classification; aorta (I707), other arteries (I708), and arteries of whole body or nonspecific lesion (I709). We excluded the code indicating aorta (I707) and included the remaining codes (I708, I709). The selected 2 codes included not only the atherosclerosis of lower extremity arteries, but also atherosclerosis of upper extremity arteries and intra-abdominal arteries. However, the prevalence of the latter is very low and deserves little consideration. The prevalence of arterial occlusive disease of upper extremities was 5%, most of them a secondary manifestation of autoimmune diseases. A true atherosclerosis of upper extremity arteries is very rare [10]. According to a study that performed duplex scans in the asymptomatic population over 65 years of age revealed 6.8% prevalence of renal artery atherosclerosis and 17.5% prevalence of mesenteric artery atherosclerosis [1112]. Symptomatic cases were rare and the incidence of acute mesenteric ischemia was 1 in 1,000 hospital admissions with only 25% of them originating from atherosclerosis [13]. The prevalence of chronic mesenteric ischemia is about 1/100,000 in the general population [13]. Upon these concerns, we have concluded that atherosclerosis of other arteries (I708) and arteries of the whole body or of nonspecific lesion (I709) are sufficient to represent atherosclerosis of the lower extremities arteries.
The present study could not analyze incidence, patency after procedure or patient survival due to data characteristics. We concentrated on the changes of patient number, patient distribution according to sex or age, total number of procedures, and procedure distribution in the recent 5 years.
This study was approved by the Seoul St. Mary's Hospital Institutional Review Board (approval number. KC13EISI0452).
RESULTS
Carotid arterial occlusive disease
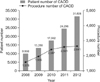
The number of patients with CAOD increased by about 30% every year (Fig. 2). When grouped according to age, the number of patients rapidly increased after the 50s and reached its peak at the 60s; 86% of patients were distributed between 50 and 79 years of age. The gender dominance was not clear in patients younger than 30 years, but the number of male patients was greater than that of female patients and accounted for 60%–65% in patients over 30 years.
From the year 2008, the number of open surgeries (OS) and endovascular treatments (ET) increased by more than 20% during each of the first two years and increased by 10% every year for 3 years thereafter (Table 2). The pattern of increment was similar between both modalities. Although the total number of procedures performed in CAOD increased over the five years, the rate of increment declined (Fig. 2). The ratio of procedures per patient decreased from 15.7% in 2008 to 8.3% in 2012. As for the preference of treatment modality, ET was preferred over OS and occupied 77%–79% of the total number of procedures. This tendency was more evident in patients aged over 80 years old and ET accounted for 82%–89% of the total number of procedures. Stent insertion accounted for 95% of ET; balloon angioplasty occupied the remaining 5%.
Abdominal aortic aneurysm
The number of patients with AAA increased by 11%–17% every year. When AAA, ruptured (I713, I715) and AAA, unruptured (I714, I716) were compared, the number of unruptured AAAs increased by 104% during the five years, while that of ruptured AAAs increased by 25% (Table 2).
The number of patients increased rapidly in patients over 50 years old, and reached its peak at the age of 70; 76%–77% of patients were distributed between 50 and 79 years of age. Male patients were dominant between 50 and 79 years of age, while female patients were dominant in patients younger than 10 years of age. The proportion of males to females was equal in patients older than 80. The total number of procedures increased by 116% in total, of which ET was especially prominent. ET occupied 52% of the total number of procedures in 2008 and gradually increased to 70% in 2012. Preference for ET was apparent in the elderly, occupying 77% of procedures performed in patients over 80.
Arterial occlusive disease of lower extremity
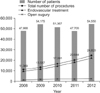
The number of patients who were diagnosed LAOD fluctuated over the five years (Fig. 3). The distribution of patients according to age was similar to that of CAOD. The number of patients increased in patients over 50 years of age and reached its peak at the age of 60s; 75%–77% of patients were distributed between 50 and 79 years of age. In contrast to the fact that CAOD and AAA in regard to age or sex did not change over the 5 years, the number of patients with LAOD increased for males and the elderly. The proportion of male patients was 57% in 2008 and 64% in 2012. Male patients were dominant in all age groups, except for patients over 80 years of age in which sex distribution was equal. The number of patients younger than 50 years declined from 17% in 2008 to 11% in 2012.
The total number of procedures increased each year by 20%– 25%. OS increased by 17%– 26% each year for the first 2 years and slowed down to 1%– 6% each year for 3 years. ET, in contrast to OS, constantly increased by 18%– 24% each year and occupied 80%– 95% of the total number of procedures in all age groups (Fig. 3).
Current trends of ET in Korea
The number of centers treating CAOD with ET increased by 31%; from 82 centers in 2008 to 108 centers in 2012. AAA was managed with ET in 37 centers in 2008 and rapidly expanded by 110% to 78 centers in 2012. One hundred twenty centers treated LAOD with ET in 2008, which increased by 36% to 163 centers in 2012.
Almost half of all ET of MADs was performed by interventional cardiologists (IC) during the study period of 5 years (Fig. 4). The other half was performed by vascular surgeons, cardiothoracic surgeons, and interventional radiologists.
The ratio of reintervention of ET calculated as the total number of interventions divided by the total number of patients treated with ET increased every year from 11.5% in 2008 to 17.6% in 2012. The frequency of reintervention was greatest in LAOD. LAOD treated with balloon angioplasty was 19.7% in 2008 and 32% in 2012 with an average of 23.3% for 5 years.
The total number of ETs performed in MAD increased by 20%–27% each year and summed up to 124% at 2012. As for coronary artery disease (CAD), it only increased by 22% during the five years (Table 2). In 2008, MAD comprised only 18% of the total number of ETs that was performed in MAD and CAD, but increased to 30% in 2012 (Fig. 5).
DISCUSSION
Over the past 5 years, patients with CAOD increased by 217%, while that of AAA and LAOD increased by 78% and 14%, respectively. Accordingly, the number of treatments increased by 124%.
The increase of PADs can be seen in both the developed countries and the underdeveloped countries, which is becoming a social-economic burden [314]. The management of LAOD with ET often requires repetitive procedures, which is likely to increase medical costs [15]. Therefore, it highly recommended that management of asymptomatic LAOD and claudications of LAOD follow guidelines [16]. The prevalence of AAA in screening data shows 4% to 7.6% [17181920]. The prevalence in Korean over 65 years of age is 3.2%, and those who require treatment with diameter over 5 cm are about 0.2% [14]. Endovascular aneurysm repair (EVAR) has lower short-term mortality and morbidity compared to open surgery, but shows similar long-term survival after 2 years [21222324]. The application of EVAR can be limited due to several factors such as anatomical feasibility and suitability of peripheral vascular access. Even so, EVAR is being preferred more and more, following the minimally invasive trend. But due to increase in need for reinterventions and surgeries after EVAR failure, the increase of medical cost is inevitable. This would be intensified with fenestrated and branched grafts, which is yet to be released in Korea.
In our study, carotid artery stenting (CAS) occupied 77%–79% which is exactly the opposite results compared with the world trends [25]. Carotid end arterectomy should still be considered as the first choice of treatment, limiting CAS to anatomically difficult lesions only [26]. Since CAS increases the risk of stroke compared to end arterectomy, this must be considered before procedure [27]. The proportion of IC was more than half of the medical providers in this study. This seems to be consistent with the fact that increment of ET in CADs was only 22% over the past 5 years, implying that ICs have moved on to treating MADs.
The role of surgery is still important in the era of ET [2829]. Considering the complexities and diversities of vascular treatments, the ability to perform both treatment methods are required to provide better results for patients.
In conclusion. it is evident that the incidence of vascular diseases will be increasing as our society ages, not to mention its care cost. The need for long-range plans and guidelines are urgent.





 XML Download
XML Download