

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Leiomyosarcomas are rare malignant smooth muscle tumors that most commonly arise from the uterus, gastrointestinal tract, retroperitoneum or soft tissue. They comprise less than 1% of all cancers and 2% to 9% of sarcomas [1]. These tumors usually grow and metastasize slowly, most commonly to the lung. Primary pulmonary leiomyosarcomas are extremely rare, accounting for less than 0.5% of all malignant lung tumors [2]. We report the case of a female patient with a history of lobectomy for pulmonary leiomyosarcoma, who presented with metastasis to the intrapancreatic common bile duct (CBD) and survived 5.5 years after the first diagnosis.
CASE REPORT
A 57-year-old female patient was referred to our department for surgical treatment of an intrapancreatic CBD tumor. The patient's past medical history was significant for hysterectomy and unilateral oophorectomy due to uterine leiomyoma ten years prior., and primary pulmonary leiomyosarcoma, which was treated with right upper lobectomy and lymph node dissection six months prior to her presentation. In order to diagnose the primary origin of the tumor, the patient underwent abdominal magnetic resonance imaging (MRI), which was negative. Histopathologic examination of the specimen revealed a malignant mesenchymal neoplasm, measuring 6 cm in greatest dimension, with morphological characteristics and immunophenotype compatible with leiomyosarcoma. Cell proliferation marker Ki-67 was positive in the majority of cells (>85%) and extensive necrosis was present. Immunohistochemical examination was positive for smooth muscle actin (SMA) and negative for S100. The neoplasm had locally infiltrated small vessels, one lymph node and the pleura.
During the next six months the patient suffered three episodes of acute cholangitis. Conservative treatment resulted in remission of symptoms. Abdominal computed tomography (CT) scan showed dilation of intrahepatic and extrahepatic bile ducts and a tumor located in the distal CBD. Chest CT scan revealed bilateral micronodural lung lesions, compatible with metastases. An endoscopic ultrasonography confirmed the existence of the tumor in the endopancreatic portion of the CBD. Bile duct brushing cytology and cytological examination of aspirated bile fluid were negative for malignancy, while biopsies taken from the mass revealed high grade malignant neoplasm, without defining its exact histological type. The patient was then referred to our department for surgical treatment.
Upon admission, physical examination and laboratory findings, including tumor markers, were normal. Under the preoperative diagnosis of periampullary tumor, pylorus-preserving pancreaticoduodenectomy was performed. Postoperative course was uneventful and the patient was discharged on the 12th postoperative day.
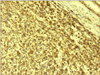
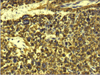
Histopathologic examination of the specimen revealed a polypoid tumor, 1.5 × 1.4 × 2 cm in size, infiltrating the full thickness of the common bile duct, extending into its lumen, without obvious invasion of the pancreatic tissue (Figs. 1, 2, 3). Tumor cell necrosis, high cellularity, many mitotic counts, pleomorphism, and nuclear atypia were present in the neoplasm. Immunohistochemical study gave positive results for HHF-35, SMA and desmin, focal positivity for CD68 and negative results for keratin 7, keratin 20, keratin AE1/AE3, careinoembryonal antigen, epithelial membrane antigen, synaptophysin, S-100, CD117 (c-kit) and CD34. Cell proliferation marker Ki-67 (MIB-1) was estimated at 40%. Morphological and immunohistochemical characteristics of the neoplasm were compatible with high grade polymorphous sarcoma with muscular differentiation. Resection margins were clear and none of the five lymph nodes found in the specimen was involved.
Soon after the second surgery, the patient was set on adjuvant chemotherapy with gemcitabine plus docetaxel for the pulmonary metastases. Effective eradication of lung lesions was never accomplished and fifty eight months after the first surgery, the patient developed bone metastases. Ten months later the patient died, five and a half years after the first diagnosis of leiomyosarcoma.
DISCUSSION
Leiomyosarcomas are rare, comprising less than 1% of all cancers. Moreover, primary leiomyosarcomas of the lung are extremely rare. These tumors tend to metastasize hematogenously, late in the disease process, most commonly to the lung [3].
When seen in the lung, it is important to establish whether a leiomyosarcoma originated in the lung or if it is secondary to metastases from a separate location, the latter being much more common. Yet, in our patient the negative abdominal MRI scan before the first surgery suggests that the CBD tumor was probably metastatic. Similarly, the bilateral pulmonary lesions detected in the chest CT scan represented intrapulmonary metastases, as they were not present before the first surgery. Despite the existence of metastatic pulmonary disease and the undetermined histological type of the tumor, the Whipple procedure was decided upon given the patient's good physical status and the fact that the CBD tumor had caused recurrent episodes of cholangitis.
Low-grade lesions and all lesions smaller than 5 cm are generally considered "cured" if adequately resected [4]. By contrast, the median survival for patients with unresectable sarcoma or metastatic disease is about 12 months [5]. Yet, large tumor size is not a precise predictor of adverse outcome. In leiomyomatous tumors, mitotic figures have been suggested to be the most important predicting parameter [6]. In our case the primary lung tumor was poorly differentiated, measuring 6 cm in diameter. Thus, despite adequate resection, development of metastatic disease was quite probable. Furthermore, histopathological features of the tumor, which were all predictive of aggressive behavior, increased the chance of recurrence [5]. Yet, the patient's survival far surpassed the aforementioned median survival.
Additional information from the patient's medical history that should be further discussed is the uterine leiomyoma. The patient denied having any written information about it, such as histological report. In effect, one cannot exclude the possibility of uterine smooth muscle tumor of uncertain malignant potential (STUMP). STUMPs are tumors that show any unusual combination of atypia, mitotic rate and type of necrosis that do not satisfy the Stanford criteria for leiomyosarcoma. Recurrence rates of 7.3% to 26.7% having been reported in the literature. Recurrence in STUMPs is often delayed, on average, 51 months. STUMPs may recur as STUMPs or as leiomyosarcomas [7]. In conclusion, we could exclude that both the lung tumor and the CBD tumor represented metastases from a STUMP, recurring as leiomyosarcoma.
To our knowledge, this represents the first reported case demonstrating metastasis from primary pulmonary leiomyosarcoma to the intrapancreatic CBD, resulting in a remarkably long survival. The authors believe that, in similar cases, surgeons should be encouraged to treat metastases surgically, even if this requires major resections.

 XML Download
XML Download