

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With global aging gaining ground in the 21th century, menopausal transition in women around the age of 50 is becoming more pronounced. With the cessation of menstruation as a sequel to the loss of ovarian follicular activity, there is a gradual decrease in estrogen and progesterone levels with an increase in follicular stimulating hormone. Consequently there is a change in the ratio of estrogen-progesterone to androgens with the influence of androgens becoming more important. As a result to this menopausal transition, many physiologic changes occur with major impact on daily life. Well known symptoms to these functional and organic changes are the vasomotor and urogenital symptoms accompanied by sleep disturbances, osteoporosis, and cardiovascular diseases and last but not least phonatory disturbances.12345 Abitbol and Abitbol6 in his study on 100 menopausal women on no hormonal therapy, has reported dysphonia in 17% of the cases namely reduction in vocal range and loss of high frequencies. In a survey by Boulet and Oddens7 using a questionnaire filled by 48 professional voice users, more than two thirds reported vocal changes around the age of 50 years, namely huskiness, loss of the high notes, reduced flexibility and stability. Scheneider et al.8 reported that 46% of women at menopause experience vocal changes and in 33% of the cases these changes are associated with vocal discomfort. The main symptoms were frequent throat clearing, dryness, and loss of certain frequencies.
Body mass Index (BMI) is an important variable that is often taken into consideration in analyzing the impact of systemic diseases such as diabetes and hypertension on various health issues in menopausal women.9 It is equally an important confounding variable while investigating the impact of lactation and multiparity on bone marrow density as reported by Sharma et al.10 and it is also an important indicator of adipose tissue content in the body, which is an important source of endogenous estrogen in post-menopausal women.11 A meta-analysis reported by Shobeiri et al.12 on the association between BMI and hot flash in midwife women revealed that obesity increases the risk of hot flash to a certain extent. On the other hand, other studies have reported that higher levels of endogenous estrogens are present in heavier women.13 To that end, it stands to reason that an increase in the amount of fat cells may result in an increase in the concentration of endogenous estrogen which may counteract the effect of menopause on voice. Based on PubMed review using “menopause” and “body mass index” as key words, only three studies have considered BMI as a confounding variable in the analysis of vocal changes associated with menopause.141516 D'Haeseleer et al.15 has initially reported a positive correlation between BMI and speaking fundamental frequency in a group of postmenopausal women not on hormonal therapy. In this group which consisted of 26 women, an increase in BMI was associated with a higher fundamental frequency. This correlation was not present in premenopausal women and in post-menopausal women on hormonal therapy. Two years later the same authors have demonstrated that menopause women with low BMI who were not on hormonal therapy had lower speaking fundamental frequency compared to pre-menopause women with low BMI.
With the paucity of reports on the phonatory symptoms and acoustic findings in menopausal women in comparison to pre-menopausal women accounting for BMI as a confounding variable in the analysis, the authors have been intrigued to compare the phonatory symptoms and acoustic variables in two groups with similar body mass composition and to investigate the correlation between BMI and the aforementioned variables. The hypothesis is that menopause women have a higher prevalence of phonatory symptoms than pre-menopause women and that high BMI may mask some of these symptoms. Acoustic analysis will also be performed in this investigation taking into consideration BMI as a confounding variable.
Materials and Methods
A total of 69 women presenting to obstetrics and gynecology clinic within a period of 6 month starting June 2015 were invited to participate in this study after having read the informed consent approved by the Institutional review board. Patients with recent history of upper respiratory tract infection, laryngeal manipulation or laryngeal surgery were excluded from this study. Given the confounding effect of hormonal therapy on voice, all those on hormonal therapy were excluded as well. Subjects were divided into two groups, 34 menopausal and 35 pre-menopausal.
Demographic variables included age, smoking, and BMI. BMI was defined as the weight in kilograms divided by the square of the height in meters (kg/m2). Subjects were classified as having low BMI, or high BMI based on a cut-off value of 25 kg/m2.17 The authors of this manuscript were keen on having equal distribution of subjects with normal BMI in the two groups given the importance of fat as a source of estrogen in females.
All subjects were asked about the presence or absence of the following symptoms: Hoarseness defined as a change in voice quality and timbre, deepening of the voice, loss of high or low frequencies, pitch breaks, throat clearing, dryness in the throat and vocal fatigue. The Voice Handicap Index (VHI)-10 by Jacobson et al.18, was filled by all the subjects.
All subjects underwent acoustic analysis using the Visi-Pitch IV by Pentax.19 Sitting in a quiet room with the microphone placed 10 cm away from the mouth patients were asked to sustain the vowel /a/ at a comfortable pitch and loudness and the following parameters were retrieved using the multidimensional voice program; fundamental frequency, habitual pitch, Shimmer, relative average perturbation, harmonic to noise ratio, voice turbulence index. By asking the patient to count to 10, the habitual pitch was measured using the real-time Pitch module.
Statistical analysis
Shapiro-Wilk test and a visual inspection of the histograms showed that the data is normally distributed. Independent sample t-test was used to compare the means of the acoustic measures between the two groups of women menopause and the premenopausal women and when comparing menopausal women with high or low BMI to premenopausal women. Pearson's χ2 test was used to analyze difference in the categorical variables including the phonatory symptoms between the two groups of women (menopausal and premenopausal women). Fisher-exact test was reported when more than 20% of the cells had a cell count less than 5. P value > 0.05 was considered non-significant.
Results
1. Demographic variables
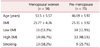
A total of 34 menopausal women and 35 pre-menopausal women were enrolled in this investigation. The mean age of menopausal women was 53.5 ± 5.57 years and the mean age of non-menopausal women was 46.69 ± 5.97 years. There was no statistical significance in the age between the two groups. Close to fifty percent of both groups had normal BMI (Table 1).
2. Prevalence of Phonatory symptoms in the menopausal and non-menopausal group
There was a significantly higher prevalence of throat clearing and dryness in the menopausal group compared to the pre-menopause group with a P value of 0.035 and 0.032 respectively (Table 2A). When BMI was taken into account, there was no statistically significant difference in the prevalence of any of the phonatory symptoms in menopausal women with high BMI and pre-menopause (Table 2B).
3. Acoustic analysis of menopausal and pre-menopausal group
There was no statistically significant difference in the means of any of the acoustic parameters between the menopausal group and pre-menopausal group (Table 3A). Similarly there was no statistically significant difference in the prevalence of any of the acoustic parameters in menopausal women with high BMI and pre-menopausal women (Table 3B).
4. VHI in menopausal and pre-menopausal women
There was no significant difference in the mean VHI-10 between the menopause group and the pre-menopause (P = 0.652). There was also no significant difference in the mean VHI-10 between the menopause group with low BMI and the pre-menopause (P = 0.435) (Table 4).
Discussion
Fat is considered as a main converting site for androgen and as such an important source of estrogen. With an increase in the amount of fat cells we anticipate an increase in the concentration of endogenous estrogens and inversely a decrease in the concentration of fat cells will result in less production of endogenous estrogens. To that end, it has been reported that women with an elevated BMI have higher estrogen levels.2021 As the larynx is a hormonal target, fluctuation in the level of sex hormone is expected to have an effect on the vocal folds and subsequently on voice. In fact, Abitbol et al.22 has shown the presence of desquamation and proliferative changes in smears taken from the vocal folds similar to the ones taken from the cervix. Cytologic findings taken from epithelial smears of cervix and vocal folds have also been shown to be similar as reported by Caruso et al.23 with marked evidence of atrophy and dystrophy in menopausal subjects not on hormonal therapy. As a sequel to these hormonal effects, there is a higher prevalence of vocal symptoms in menopause women compared to premenopausal women. The prevalence varied between 17% to 77% based on the methodology used and subjects investigated. The most common reported symptoms are dryness, frequent throat clearing, vocal fatigue, roughness, loss of range, and deepening of the voice.2224 These symptoms seem to be more pronounced in professional voice users compared to non-professional voice users and are often referred to as the “post-menopausal vocal syndrome”. This discrepancy in prevalence can be attributed to the increase in vocal demand among professional voice users in addition to their increase awareness.21 Those with high prevalence of phonatory symptoms were found to have muscular atrophy of the vocal folds, presence of microvarices, thinning of the vocal fold mucosa and loss of its white appearance among other videolaryngostroboscopic findings.22 Similarly in a study by Schneider et al.8 on 24 menopausal females, almost most women with vocal complaints had viscous mucosa on videostroboscopy and 50% had either edema or swelling of the vocal folds compared to normal laryngeal findings in those with no complaints.
Only few studies, namely the ones by D'Haeseleer et al.15 have investigated the phonatory symptoms and acoustic changes in menopausal women taking into account BMI as a confounding variable. In several studies there was a correlation between BMI and speaking fundamental frequency.121314 There was no mentioning of the prevalence of phonatory symptoms and their correlation with BMI. The results of this study corroborate the correlation between voice and BMI in menopausal women further substantiating the role of fat in as an important confounding variable in the prevalence of these symptoms. The analysis revealed higher prevalence of throat clearing and dryness in the overall menopausal group compared to the pre-menopausal group. When BMI was taken into consideration, menopausal subjects with high BMI did not have higher prevalence of any of the phonatory symptoms compared to pre-menopause women. This can be explained on the basis that fat is an alternative endogenous source of estrogen that can mitigate or mask the effect of menopause on voice as explained at the start of this discussion.
More often than not the perceptual vocal changes reported by menopausal women are substantiated by acoustic findings such as a low fundamental frequency, a contracted range, a reduction in maximum phonation time and an increase in perturbation parameters namely shimmer and jitter.2223 In the study by Schneider et al.8 phoniatric evaluation performed on only 24 subjects revealed a reduction in the lower frequency range in the group with complaint and a lower fundamental frequency for the habitual speech in both groups, those with and without vocal complaints. Likewise in a study by Raj et al.25 there was statistical difference in the fundamental frequency and range between menopausal women and reproductive women. On the other hand there were several studies by Meurer et al.26 and Mendes Laureano et al.27 that failed to show any significant differences in the fundamental frequency and cycle to cycle variations parameters namely shimmer and jitter for the vowels /i/ and /e/. Similarly a study by Mendes L showed no significant difference in any of the perturbation parameters in postmenopausal women vs non menopausal ones. Our study is in agreement with the aforementioned studies that failed to show any statistical significant difference in the acoustic parameters between the menopause group and the pre-menopause group.
The clinical significance of this study lies in the subject selection where both BMI and age were taken into consideration. The results are in accordance with the few reports supporting the importance of fat when investigating the effect of menopause of voice. Nevertheless there are two limitations to this study: One is the rather small subject sample and two is the lack of laryngeal examination. A larger sample size may have further substantiated the mitigating effect of high BMI on voice in menopausal women.
Conclusion
Menopausal women have more throat clearing and dryness compared to pre-menopausal women. When BMI is taken into account these symptoms were absent in the menopausal group with low BMI compared to the pre-menopause. These results corroborate previous reports on the effect of menopause on voice and substantiate the importance of fat as an alternative source of estrogen which can mask some of the phonatory symptoms.





 XML Download
XML Download