

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Osteoporosis causes high social and economic costs to the society and thus is a critical problem of concern amongst the elderly especially.1 Incidences of osteoporotic fractures are known to happen more frequently in the elderly than in the young. However, osteoporosis is diagnosed based on the bone mineral density (BMD) retrieved from dual energy X-ray absorptiometry (DXA) scans. This is a problem as the diagnosis is often inaccurate in identifying people with and without osteoporosis. Many who obtain a fracture have not been diagnosed with osteoporosis previously. A study has shown that only 48% of patients who were diagnosed as osteoporotic, experienced hip fractures.2 Furthermore, amongst patients who were treated with risedronate, a drug of interest in this study, only 40% of the osteoporotic patients and 30% of the elderly patients had decreased fracture risk.3 This goes to show that BMD only partially reflects hip fracture risk.4,5
While BMD itself has several inherent limitations, the main criticisms can be summarized as follows; it is obtained from a single areal projection in one plane and consequently cannot be characteristic of overall three-dimensional bone mass distribution.6 Secondly, the non-uniform geometry of the bone renders averaged or mean parameters less useful as they could mask the net gain or loss of bone mass. Lastly, we also overestimate the capability of BMD to be a substitute for geometry and strength which can be an ambitious task from a single predictor.
During the course of our study, we observed that changes in BMD across a follow-up study likes ours was meaningless as an increase in BMD due to drug treatment did not represent an improved structure. Instead, we found local regions of osteoporosis, or in other words, extreme loss of bone mass in localized regions. Therefore, we analyzed local buckling ratio (BR) values in the femoral neck (FN) over three years in risedronate treated patients, which is a common bisphosphonate, used to treat osteoporosis. And these BR values were then used to characterize finite element predicted fracture loads and thus discover regions of local osteoporosis. And this pathogenic existence of local osteoporosis could mean a higher risk of FN fracture despite drug treatment.4
Materials and Methods
As this study aims to understand the local geometric instabilities in the FN, two subjects were analyzed in details. These two subjects were administered risedronate drug treatment, over three years from 2008 to 2010. To compare the geometries of their FNs, BR was calculated. This was attained by measuring the outer radius and the cortical thickness at twelve different intervals along the cross section of the FNs.7 Commercial software, Mimics® (Materialise, Leuven, Belgium), was used to extract these geometric values. BR is given as the ratio of the mean outer radius to the mean cortical thickness.8 Therefore, prior to averaging the outer radius and cortical thickness values obtained at the twelve intervals, BR is calculated. Consequently, a BR value for each year (2008, 2009 and 2010) for each of the two subjects was obtained. Through use of finite element analysis, we obtained the critical fracture load (Fcr) which was used as the ultimate point in which failure occurs in the femur and in particular, the FN. Also, a Fcr was derived from finite element analysis, using commercial software, ABAQUS® (Dassault Systèmes Simulia Corp., Providence, RI, USA).9
Results
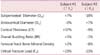
Subject #1 was a 73 year old Korean female with a body mass index (BMI) of 26.1 and FN BMD of 0.628 in the baseline year, whereas subject #2 was a 75 year old Korean female with a BMI of 26 and FN BMD of 0.594 (Table 1). Both subjects were in the same age group with little difference in their BMI and a 3.4% difference in their FN BMD,10 which is insignificant. Thus, the comparison of their geometrical and structural parameters is a fair one.
As shown by Table 2, mean geometrical properties, FN BMD and Fcr of the two subjects are tabulated. It can be seen that Subject #1 exhibited an increase in Fcr (+23%), with an increase in periosteal diameter and no change in endocortical diameter, consequently reflecting an increase in mean cortical thickness (+37%). While FN BMD did not show a significant change from 2008 to 2010 (+2%), the overall BR seems to show an unexpected increase (+5%). In contrast, subject #2 exhibited a decrease in Fcr (-23%), with a decline in the subperiosteal diameter (-18%) and an increase in the endocortical diameter (+7%). Due to this unmatched changes, the mean cortical thickness declined (-9%) which seems to be matched by a similar decline in FN BMD (-8%). Also, overall BR only changed by -1%, which was insignificant.
The study then proceeded to observe the local changes in periosteal diameter, endocortical diameter, cortical thickness and BRs. While the radar plot of BRs of subject #1 shows a uniform annular structure with no abrupt changes in cortical thicknesses, the computed tomography-scan image shows limited information due to lack of resolution (Fig. 1). However, subject #2 exhibited critical regions at the supero-anterior region (30°) and a largely thick cortice at the infero-anterior region (300°-330°) (Fig. 1). In addition, plots of local BR values against the respective regions again emphasizes the fact that subject #1 had local BR values well below the critical value of 10 in 2008 and 2010 while subject #2 had a critical region in the infero-posterior region (210°-240°) in 2008 and that critical region passed on and a new one formed in the supero-anterior region (0°-60°) in 2010 (Fig. 2).
Discussion
In this study, the structural parameter predicted from finite element analysis was analyzed together with the derived geometric parameter, to observe any patterns or correlations, which may provide more insight in the etiology of FN fractures. The penultimate aim is to work towards a more rigorous diagnosis. By observing more predictors with localized changes, with the inclusion of geometry and strength in the diagnosis through use of imaging and finite element analysis, this aim could be achieved.
With respects to both subject #1 and subject #2, it was found that the changes in the overall BR were insignificant. This was because an increase in BR is supposed to reflect cortical instability and vice versa. This would mean that the overall BR for subject #1 should decrease while for subject #2 it should increase, based on their respective fracture load changes. This shows that other than the mean cortical thickness,11 which seems to correlate with changes in Fcr, the changes in the other mean geometrical parameters as well as FN BMD did not provide any useful information. This warranted a look at the local BRs.
Despite the fact that both subjects were under antiresorptive drug treatment, only subject #1 has shown a positive response as there were no critical regions of extremely thin cortices. On the other hand, subject #2 has shown a negative response. This is because although, the critical region at the infero-posterior region disappeared, another critical region formed at the supero-anterior region. This suggests that the drug treatment could be more effective in selective regions, for example, at regions with higher loadings, in response to greater mechanical demands.10
Hence, the findings prove the importance of patient-specific analysis. Patients may already be facing a pathogenic existence of local osteoporosis that may compromise on their anti-resorptive drug treatments.4 By assessing their radiological scans, and with the help of radar plots as shown in this study, detailed observations can be made on their FN regions and appropriate exercise strategies that provide increased loadings at the critical zones can be implemented that would benefit the patients more than just the administration of drug treatment.



 XML Download
XML Download