

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Erythrophagocytosis by monocytes or macrophages is occasionally seen in hematologic malignancy, autoimmune hemolytic anemia, and hemophagocytic lymphohistiocytosis [12]. However, erythrophagocytosis by neutrophils on the peripheral blood smear is an unusual morphological phenomenon. Erythrophagocytosis by neutrophils has been reported in patients with some hemolytic anemias, particularly paroxysmal cold hemoglobinuria (PCH), and other conditions including poisoning with potassium chlorate, sickle cell disease, and incompatible transfusion [3456]. Cases of erythrophagocytosis by neutrophils have rarely been observed in cold agglutinin disease (CAD) [789]. We report a female patient with CAD and the presence of erythrophagocytosis by neutrophils on the peripheral blood smear.
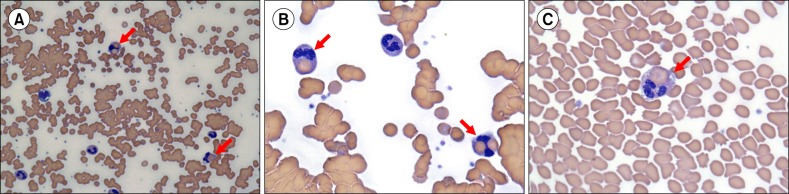
An 80-year-old woman was referred to our hospital because of dizziness. A few days prior to referral, she had cold symptoms, with a cough and rhinorrhea. She had a history of hypertension. Physical examination revealed icteric sclera and jaundice of her torso. Her white blood cell count was 15.88×109/L (83% segmented neutrophils, 8% band forms, 1% metamyelocytes, 2% myelocytes, 3% lymphocytes, and 3% monocytes), hemoglobin concentration was 9 g/dL, and platelet count was 369×109/L. Other laboratory tests showed the following: increased lactate dehydrogenase (2,530 IU/L), total bilirubin (5.14 mg/dL), and direct bilirubin (2.05 mg/dL), and decreased haptoglobin (2 mg/dL). The peripheral blood smear showed red blood cell (RBC) agglutination with a few nucleated RBCs and erythrophagocytosis by approximately 10% of the neutrophils (Fig. 1). Cold agglutinin titer was 1:256. The direct Coombs' test returned positive results (3+) for C3d and weakly positive results for IgG. The indirect Coombs' test returned negative results. Sepsis was suspected and empirical was administered. However, the patient's condition deteriorated rapidly and she died two days after admission. Although the Donath-Landsteiner test was not examined and PCH could not completely be excluded, a diagnosis of CAD was made based on the available laboratory results.
CAD is generally classified as primary (idiopathic) or secondary. The latter is associated with underlying conditions such as malignancy, infection, or immune disorders [10]. Therefore, after diagnosis of CAD, patients should be evaluated for underlying conditions. Two sets of blood cultures returned negative results. Mycoplasma pneumoniae and Epstein-Barr virus were not detected. Evaluation for underlying malignancy or other disease was not performed because of the short clinical course. Therefore, we could not determine whether underlying disease was associated with the CAD.
The CR1 receptor of neutrophils can react with RBC-bound C3b [11]. However, the mechanism underlying erythrophagocytosis by neutrophils is unclear. To the best of our knowledge, this is the first reported case in Korea of CAD with erythrophagocytosis by neutrophils on a peripheral blood smear.
 XML Download
XML Download