

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
Catabacter hongkongensis, a newly described anaerobic Gram-positive coccobacillus pathogen, was first isolated in 2007; its draft genome sequence was revealed in 2015 [12]. C. hongkongensis infections are rare, mostly occurring in Hong Kong, but clinically relevant, presenting as sepsis resulting from gastrointestinal disease [12].
A 77-yr-old man was admitted to the hospital for febrile sensation and abdominal pain. Eight years previously, he underwent endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic sphincterotomy for acute cholangitis with a common bile duct stone. He also had a history of hypertension, diabetes mellitus, dilated cardiomyopathy, and atrial fibrillation. Physical examination revealed tenderness over the right upper quadrant of the abdomen, and a diagnosis of acute cholecystitis was made. Laboratory parameters were as follows: leukocyte count, 11.3×109/L (neutrophils, 90.9%); Hb, 16.3 g/dL; platelet count, 113×109/L; AST, 96 U/L; ALT, 52 U/L; alkaline phosphatase, 84 U/L; γ-glutamyl transpeptidase, 163 U/L; total bilirubin, 3.35 mg/dL; direct bilirubin, 1.68 mg/dL; and C-reactive protein, 8.6 mg/dL. Coagulation profiling revealed prolonged prothrombin time (PT, 23.0 sec) and activated partial thromboplastin time (aPTT, 54.1 sec) due to warfarin treatment. Abdominal CT showed gallbladder stones, edematous thickening of the gallbladder wall, mild dilatation and pneumobilia in the left intrahepatic bile duct. The day after admission, ERCP and endoscopic retrograde biliary drainage was performed. Hemobilia originating from the gallbladder was detected, but an emergency operation could not be performed because of prolonged PT and aPTT.
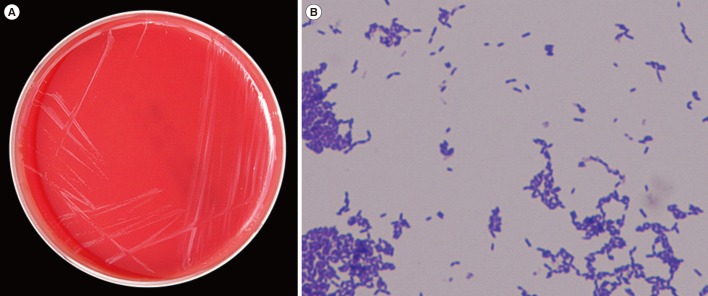
Two blood cultures were obtained, and treatment with empirical intravenous cefodizime and metronidazole was initiated. On day 3 post-incubation, Gram-positive coccobacilli were isolated from the two anaerobic blood cultures. These organisms grew on sheep blood agar as non-hemolytic, white, pinpoint colonies after 48-72 hr of anaerobic incubation at 37℃ (Fig. 1). The bacteria produced catalase. The isolate was not identified by phenotypic identification methods using the Vitek2 ANC card (bioMérieux, Marcy l'Etoile, France) or the API 20A system (bioMérieux). Two matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry instruments, a MALDI Biotyper (Bruker Daltonics Inc., Billerica, MA, USA) and a VITEK MS (bioMérieux), also could not identify the isolate. We therefore sequenced the 16S rRNA gene for identification at the species level [3]. The 16S rRNA sequences (1,358 bp) showed 100.0% similarity with the sequence of C. hongkongensis strains (GenBank accession no: LT223646.1, AB671763.1, NR_115269.1). There were some differences in the biochemical test results of the isolate from that of genetically similar organisms: Ruminococcus species (GenBank accession no: AJ318864.1) that showed Gram-positive diplococci and catalase negativity and Christensenella species (GenBank accession no: LT223568.1) that showed Gram-negative bacilli. Thus, the pathogen was identified as C. hongkongensis.
Antimicrobial susceptibility testing was performed by E-test strips (bioMérieux) or disk diffusion method on Mueller–Hinton agar. Categorical interpretation according to CLSI breakpoints was used. The isolate was susceptible to vancomycin (minimum inhibitory concentration [MIC] 0.5-0.75 µg/mL) and metronidazole, but resistant to penicillin, cefotaxime (MIC>32 µg/mL), colistin, and gentamicin (MIC>256 µg/mL). After seven days of antibiotic treatment, the patient was discharged, and his operation was scheduled at the time of next admission. The patient underwent elective laparoscopic cholecystectomy and recovered without any complications.
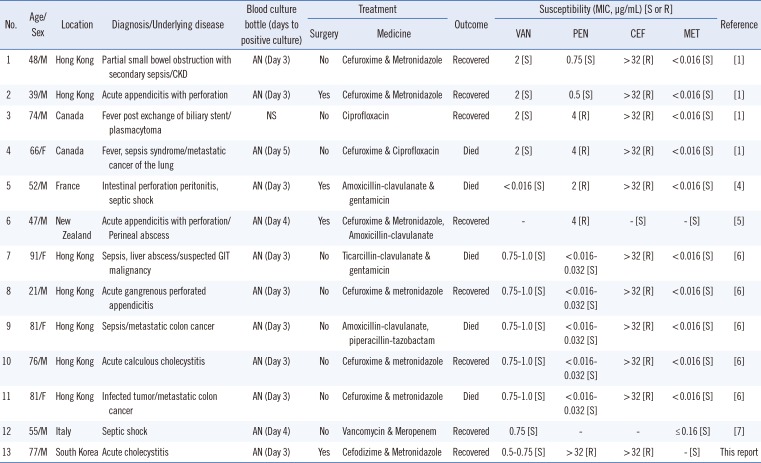
C. hongkongensis has been recently described as a pathogen capable of causing bacteremia [1]. Only twelve cases of bloodstream infection with this organism have been reported to date (Table 1) [14567]. This patient recovered rapidly with antimicrobial therapy and surgery, but five of the 12 reported cases of C. honkongensis bacteremia were fatal. Considering that C. hongkongensis bacteremia is often associated with complications and high mortality, especially in patients with advanced malignancies [6], the importance of accurately identifying this microorganism should be highlighted in clinical microbiology laboratories. Our isolate was susceptible to vancomycin, similar to the isolates reported by Lau et al [6] in 2012. Six out of the seven (86%) patients who were treated with a combination of metronidazole and cefuroxime or cefodizime recovered, whereas four out of the 6 patients who had poor prognosis, i.e., death, were treated by other modalities. These results support the claim that metronidazole-based combination therapy with cefuroxime or cefodizime could be effective for treating C. hongkongensis bacteremia. Because phenotypic identification of C. hongkongensis is difficult and unreliable, the prevalence of infections caused by this organism is likely to be underestimated. Therefore, systemic gram-positive bacilli should not be ignored, and 16S rRNA gene sequencing is a unique technique for accurate species-level identification of C. hongkongensis.
 XML Download
XML Download